Thyroid gland is producing too much thyroxin hormone (overactive).
This refers specifically to excess production and secretion of T3 and T4 from the thyroid gland, disproportionate to requirement.
Specifically characterised by increased synthesis and secretion of thyroid hormones from the thyroid gland.
Thyrotoxicosis
The clinical manifestation of symptoms owing to excess T3 and T4 action in peripheral tissues (outside thyroid gland).
It is classified according to its cause of and origin of dysfunction, which can be either within the thyroid or from other tissues.
It can occur without the presence of hyperthyroidism, in response to acute autoimmune inflammation destruction of thyroid follicles, which is known as thyroiditis.
Kalhan A, Page M. Thyroid and parathyroid disorders. In: Whittlesea C, Hodson K, eds. Clinical Pharmacy and Therapeutics. London: : Churchill Livingstone 2018. 744–61.
Thyroxine levels should be checked annually by your doctor and more regularly if poorly controlled.
Cause
Family history conditions:
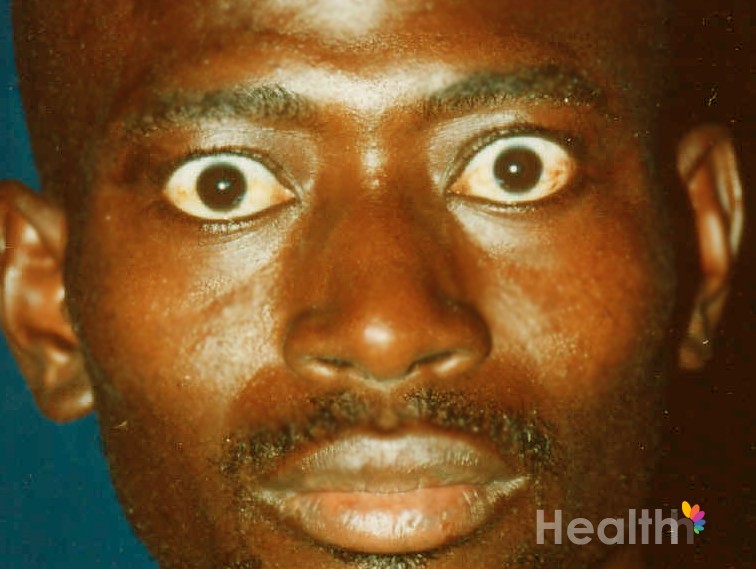
Graves’s disease (hyperthyrodism):
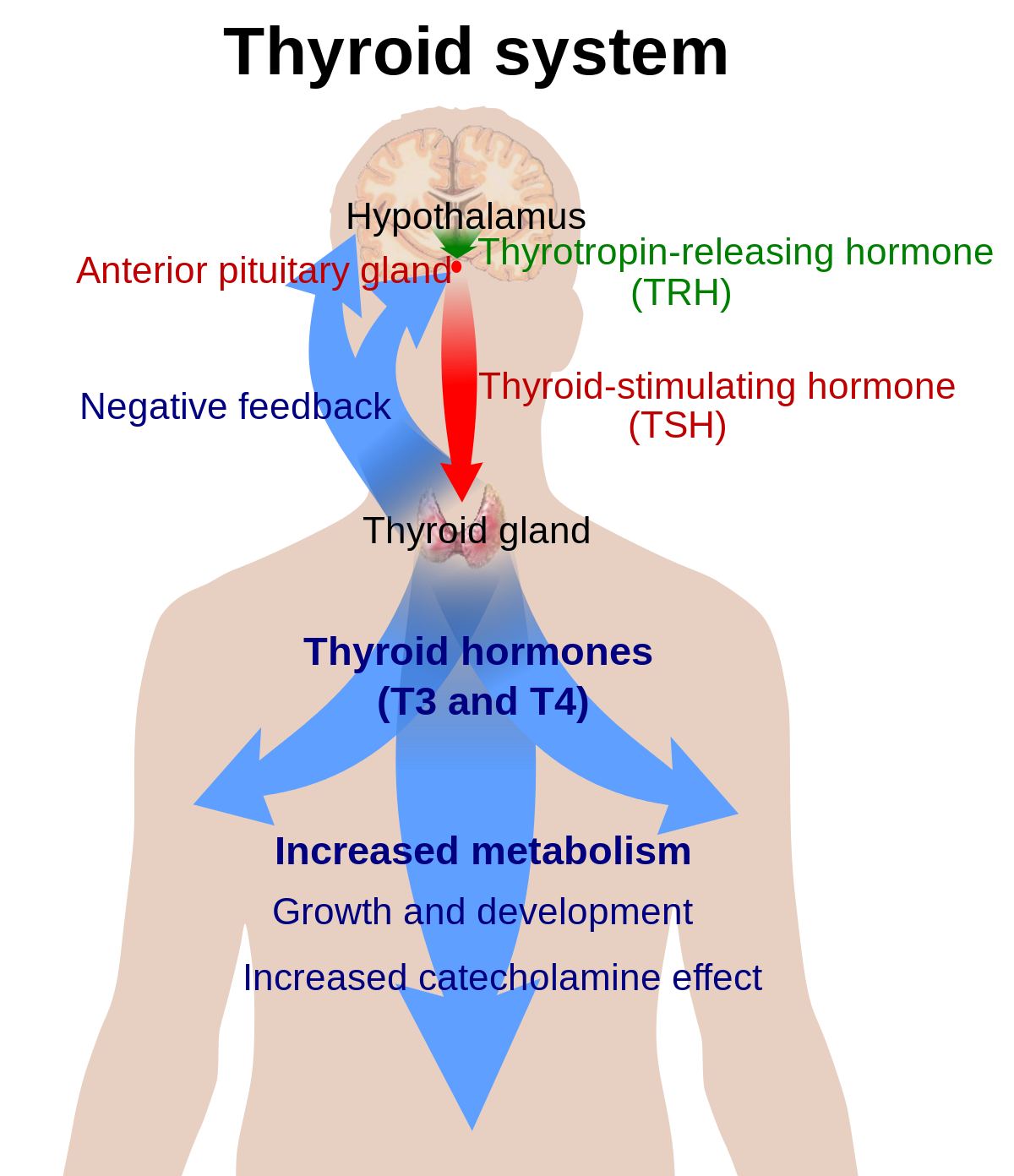
An autoimmune condition where immune system attacks it own body and inappropriately produces antibodies, known as thyroid stimulating antibodies (TSI), these antibodies overstimulate your thyroid gland and cause it to overproduce thyroid hormone.
This results in increased T3 and T4 levels (this is the hormones released by our thyroid) and suppression of TSH (this is the hormone that stimulates the thyroid gland via the brain).
Graves disease is more common among females, with a peak incidence at age 10-15 years.
Thyroid nodular disease (hyperthyroidsim):
This can be multinodular, leading to swelling or formation of a lump at the front of the neck known as a goitre, which accounts for 15–20% of cases, or a single nodular adenoma, which is found in 5% of hyperthyroid patients.
Hashimoto’s thyroiditis (thyrotoxicosis): [where the body produces thyroid-attacking antibodies including thyroid peroxidase antibodies (TPO) and thyroglobulin antibodies (TgAb) Inflammation causing hot, red and swelling and in time causes destruction of the thyroid gland leading to hypothyroidism however it can also cause periods of overactivity leading to hyperthyroidism , the main symptom is a swollen neck].
Postpartaum thyroiditis (high thyroid levels just after childbirth)
Postradiation thyroiditis (high thyroid levels after radiation exposure)
De Quervain thyroiditis (high thyroid levels causing a painful swelling of the thyroid gland thought to be triggered by a viral infection, such as mumps and/or cold and flu infection)
Toxic Multinodular Goiter – disease where the thyroid gland develops multiple nodules and enlarges (goiter), the nodules also release thyroid hormones.
Toxic multinodular disease
Pituitary-induced hyperthyroidism—where the thyroid gland can become overstimulated by the pituitary gland and produce excessive amounts of thyroid hormone.
Any disorder where the thymus gland may be small or missing (the thymus gland is beneath the breastbone, is where T cells — a type of white blood cell — mature. Mature T cells are needed to help fight infections).
Adenoma Toxic thyroid nodules (Lumps develop in thyroid gland)
Toxic multi nodular goitre (Jod-Basedow phenomenon)
Patients with myxoedema coma require admission to an intensive care or high-dependency unit for careful monitoring and treatment.
Mechanical ventilation will be required if there is significant hypercapnia or hypoxia. Non-invasive ventilation such as continuous positive airway pressure (CPAP) may used.
Hypovolaemia, hypoglycaemia and electrolyte disturbances should be corrected.
Cardiovascular status should be carefully monitored:
Pressor agents and inotropes should be avoided, as they provoke arrhythmias.
Hypothermic patients should be warmed slowly without the use of warming blankets, as peripheral vasodilatation may aggravate or induce hypotension.
Specific measures
As the numbers of patients with myxoedema coma are relatively small, there are few clinical trials regarding the treatment of these patients.
Thyroid replacement therapy
Immediate intravenous thyroid replacement is mandatory. Gastrointestinal absorption is compromised.
There is controversy as to whether this should be T4 alone, combined with T3, or T3 alone.
It is most common in adults to use T4 alone, with an initial loading dose of intravenous T4 of 100-500 micrograms. This is followed by a dose of 75-100 micrograms per day until the patient is able to take oral replacement.
It may be combined with T3 in younger patients with lower cardiovascular risk.
Antibiotics
In view of the fact that many patients will have had their condition precipitated by infection, many advocate adding a broad-spectrum antibiotic to the treatment regime.
Corticosteroids
It should be assumed that all patients have adrenal insufficiency secondary to hypopituitarism until this can be ruled out, and all patients should receive intravenous hydrocortisone at a dose of 100 mg every eight hours until the results of the random cortisol level prior to treatment are available.
The treatment strategy for thyroid storm can be divided into four general categories, including:
Treatment targeted against thyroid hormone creation and release.
Treating your body systems and tissues, such as your heart, that are affected by the excess thyroid hormone.
Treatment of the situation or illness that caused your thyroid storm.
Other supportive treatments to help with symptoms and side effects.
Medications and treatment therapies for thyroid storm can include:
Antithyroid medication (thionamides) to stop your thyroid from making new thyroid hormones.
Iodine solution to stop your thyroid from releasing thyroid hormone.
Beta-blockers to manage your symptoms.
Bile acid sequestrants to prevent your gut from reabsorbing thyroid hormone.
Acetaminophen and cooling blankets to lower your temperature.
Respiratory treatment, such as supplemental oxygen.
If you have thyroid storm, you’ll likely be in the intensive care unit (ICU) of the hospital so your healthcare team can monitor your symptoms and condition frequently.
Please see your medical doctor even if display some symptoms as as symptoms can vary from individual to individual
Detailed Information
Please copy and paste any key words from the title: Hyperthyroidism (Grave’s Disease) in the following respective 'Medtick References and/or Sources' to find out more about the disease (this also may include diagnosis tests and generic medical treatments).
The Pharmaceutical Journal covers analysis, features, opinion, learning and careers articles, providing insight and knowledge about drugs, pharmacy practice, medicines use and healthcare policy in the context of the pharmacy profession and pharmaceutical science.