Complication of the foot related to diabetes and Alzheimer disease include:
Damage to nerves (neuropathy)
When nerves in the extremities are damaged, it is not fully understood but it is believed blood supply of the nerves are disrupted.
This condition can lead to foot ulcers.
The most common form of PN is distal symmetrical polyneuropathy.
This involves the sensory, motor and autonomic nerve fibres, where the earliest changes tend to occur most distally (i.e. in the digit/fingers and progress to finger joints).
Sensory neuropathy
Where one has no feeling of pain and thermal (heat) perception.
The patient is, therefore, unaware that they cannot appreciate the sensation of pain and, thus, are unaware that an injury has been sustained.
As a result, foot pathologies such as corns, calluses, thickened nails and foot deformity i.e. bunion all pose a risk.
Without pain sensation, these pathologies may be left unnoticed (and therefore untreated), causing underlying tissue damage and ulceration.
Autonomic neuropathy
Which affects involuntary functions, such as thermo-regulation (heat control regulation) and sweat production.
Damage to these nerves leads to lack of adequate moisture in the skin, which results in loss of elasticity, dry skin, callus and fissuring (cracks on skin appear).
It also sends oxygen filled blood away from the feet depriving the foot tissue the necessary nutrients that all muscles tendons and skin tissues needs
Diabetic peripheral neuropathic pain (DPNP)
Occurs often at night
Patients complain of paraesthesia (burning or prickling sensation that is usually felt in the hands, arms, legs, or feet).
Shooting pains down the legs,
Piercing and/or stabbing pains
Burning sensation
sensitive skin and sensitivity pain
Extremely sensitive to touch pain
Metatarsalgia- a condition in which the ball of your foot becomes painful and inflamed.
Sensations of cold or warmth
Peripheral arterial disease (PAD)
Where one has an inadequate blood supply to the lower limb, decreases peripheral tissue viability and increases the skin’s susceptibility to minor trauma, impairs wound healing and increases the risk of infection.
Symptoms include cold feet, pale skin , sores on feet.
If not caught early, it can result in necrosis , foot ulcer or gangrene and loss of limb
Foot deformity
Motor neuropathy
Affects the nerves that control movement.
This results in wasting of the intrinsic muscles of the foot.
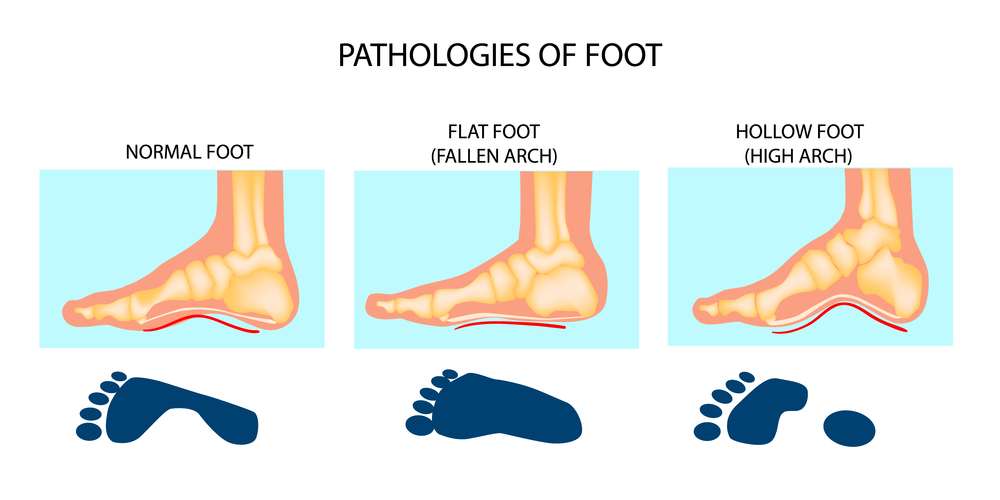
Leading to a cavoid foot:
Presents as a high arched foot with clawed toes, causing increased pressure to be placed on metatarsal heads and apices of (toes), which results in callus formation and, thus, further pressure distribution, disruption and risk.
X-ray of later stage Charcot foot, described as ‘rocker-bottom type foot’, where there is ‘disorganisation’ of the bone that results in deformity. The inset image shows the initial stages of Charcot foot, where the foot presents as red, hot and swollen.
ent (circulation assessment)
The pulses in the foot must be tested. is there a pulse on (locations include):
The dorsalis pedis (DP) is found dorsally between the first and second metatarsal shafts and the tibialis posterior (PT) is found behind the medial malleolus?
Capillary filling time:
Pressure applied to the skin on the apices of digits (toes), enough to blanch and a return of normal colour, should occur within five seconds?
Slower rates may indicate inadequate blood flow?
No blanching in a cyanotic foot is a dangerous sign and gangrene may follow?
Nerves testing
The 10g monofilament
The Ipswich touch test
Devised to be able to assess for neuropathy without the use of aids (e.g. a monofilament), which could be a barrier for testing for neuropathy in some areas.
Using the index finger, light touch is applied to the apex of the first, third and fifth toes on both feet.
If two or more sites are not felt, the patient is considered to have neuropathy
Rayman G, Vas PR, Baker N et al. The Ipswich Touch Test. A simple and novel method to identify inpatients with diabetes at risk of foot ulceration. Diabetes Care 2011;34(7):1517–1518. doi: 10.2337/dc11-0156
Complications /Information to beware of/General tips:
Table 1: Assessing a patient’s risk status for developing a diabetic foot problem
Risk status
Recommended review
Low risk
No risk factors present except callus
Annual
Moderate risk
Deformity
or neuropathy
or non-critical limb ischaemia
3–6 months with foot protection service
High risk
Previous ulceration
or previous amputation
or on renal replacement therapy
or neuropathy and non-critical limb ischaemia together
or neuropathy in combination with callus and/or deformity
or non-critical limb ischaemia in combination with callus and/or deformity
1–2 months or 1–2 weeks if have a concern with foot protection service
Active diabetic foot problem
Ulceration
or spreading infection
or critical limb ischaemia
or gangrene or suspicion of an acute Charcot arthropathy, or an unexplained hot, red, swollen foot with or without pain
Refer the person within 1 working day to the multidisciplinary foot care service or foot protection service (according to local protocols and pathways; also see recommendation) for triage within 1 further working day
Foot advice
Advising patients to check their feet daily;
Advising patients to apply moisturising cream to dry areas but not between the toes;
Advising patients to choose footwear that accommodates the shape and size of the foot to prevent rubbing or shearing;
Advising patients never to walk barefoot (to prevent standing on anything that could traumatise or injure the foot);
Advising patients to seek early advice as soon as a foot problem is identified (the National Diabetic Foot Care Audit demonstrates that this leads to shorter healing times and reduces the likelihood of amputation);
Asking the patient if they have had a recent foot check as part of their annual assessment and, if they have not, advising them to have one, as well as how to perform daily foot checks themselves.
Daily foot checks and footwear advice
Check feet daily;
For patients with reduced mobility or flexibility, using a mirror can be helpful to check the foot for changes. Alternatively, asking a friend or relative can be beneficial;
Be aware of loss of sensation;
Look for changes in the shape of the foot;
Look for discolouration of the foot;
Do not use corn removing plasters or blades;
Look after toenails and ensure these are cut straight across;
Wear shoes that fit properly;
Examine shoes for sharp objects or stones before putting them on and replace ruffled innersole linings;
Avoid socks, stockings or tights with wrinkles or prominent seams, or socks with holes or darned areas;
Garters and stockings or socks with elastic tops should be avoided because they may restrict the circulation;
Attend annual foot reviews.
The Pharmaceutical Journal,
The diabetic foot;
Online:DOI:10.1211/PJ.2017.20203299
General tips
Hot baths and massage
Some diabetics cannot tell if their skin feels hot or cold sensations (peripheral neuropathy) and may burn their skin leading to skin infection and/or a serious muscle breakdown called rhabdomyolysis.
Hot baths can increase blood flow and may reduce blood glucose levels in one’s blood due to an increase in insulin levels produced by ones body.
Massages are fine if one has no poor circulation, it is not fine if one has poorly controlled or advanced diabetes and/or is prone to muscle breakdown this can lead to numbness, heart problems and/or kidney failure as well as a serious muscle breakdown called rhabdomyolysis.
Avoid massaging areas when one has insulin injected as the pressure in the area may influence the way their body absorbs the shot and their alter their intake.
Excessive heat can can cause your heart to beat faster which may be of concern if one has an underlying heart issue/cardiovascular issue.
Foot care Patient Advice (especially diabetics or with poor foot circulation)
Look at feet each day. If you are not able to check if someone else can, particularly if you have reduced sensation in feet.
If you get a cut, bruises, redness, blister bleeding; please see your medical doctor, in the meantime cover it up with a clean dry dressing.
If you have dry skin, use a moisturising cream or oil but do not use between toes (one may have athletes foot or be at risk).
Cut your nails along curvature with toe nail clippers, not straight across. Do not damage your skin.
Wash feet regularly everyday in warm soapy (anti-bacterial soap) and/or salty (antiseptic) water especially between toes and ‘pat dry’ thoroughly.
Try to avoid foot burns:
Check bath temperature with hand before you put your feet in.
Keep your feet away from hot objects e.g. hot water bottles, electric blankets, close to fire, hearers
Avoid slip on shoes
Avoid top flat shoes, pointy shoes (have broad front with room for toes, sandals and flip flops that cause rubbing).
Always feel inside shoes for stones or rough edges before you put them on.
Always wear comfortable low heel shoes/trainers, (heels too low can strain the foot arch, cause sore and cracked heels)
Make sure they fit well (comfortable fastening, liner and buckles to prevent rubbing otherwise can get blisters). Take into account any corns, bunions, awkward shape. (If have no choice, consider specially fitted shoes to take account of bunions, corns deformities)
When buying new shoes, wear your usual socks.
Gradually break in new shoes.
Always wear comfortable socks (not too tight) with footwear. Socks protect you from a rubbing shoe.
Do not walk bare foot anywhere. One may damage their feet.
Rotate ones ankles move feet up and down and do regular feet exercise to improve suppleness and blood circulation.
Please talk to your healthcare professional (i.e. Medical Doctor/Pharmacist) for further advice
Detailed Information
Please copy and paste any key words from the title: Diabetes and/or Alzheimer’s related foot problems in the following respective 'Medtick References and/or Sources' to find out more about the disease (this also may include diagnosis tests and generic medical treatments).
The Pharmaceutical Journal covers analysis, features, opinion, learning and careers articles, providing insight and knowledge about drugs, pharmacy practice, medicines use and healthcare policy in the context of the pharmacy profession and pharmaceutical science.