Pregnancy can be ruled out with reasonable certainty if one or more of the following criteria are met and there are no symptoms or signs of pregnancy:
She has not had sexual intercourse since her last period, or since childbirth, abortion, miscarriage, ectopic pregnancy or uterine
evacuation for gestational trophoblastic disease.
She has used a reliable alternative method of contraception correctly and consistently (note that barrier methods are considered
reliable, providing that they have been used consistently and correctly for every episode of intercourse).
She is within the first 5 days of the start of a normal (natural) menstrual period.
She is less than 21 days after giving birth (non-breastfeeding women).
She is fully breastfeeding, not having periods and less than 6 months after giving birth.
She is within the first 5 days after abortion, miscarriage, ectopic pregnancy or uterine evacuation for gestational trophoblastic disease.
She has had a high-sensitivity urine pregnancy test (able to detect human chorionic gonadotrophin [hCG] levels around 20 mIU/ml)
performed at least 3 weeks after the last episode of unprotected sexual intercourse, and it was negative.
Being underweight (BMI <19) doubles the risk of having a growth-restricted baby.
Denison FC, Norwood P, Bhattacharya S et al. Association between maternal body mass index during pregnancy, short-term morbidity, and increased health service costs: a population-based study. BJOG 2014;121:72–82. doi: 10.1111/1471-0528.12443
Make sure one has folic acid, Iron and Vitamin B12, vitamin D in their diet.
Table 1 provides recommendations of daily amounts of nutritional supplements for women with a normal BMI and obese women.
Table 1: Daily dietary requirements of nutrient supplements for women
The National Institute for Health and Care Excellence (NICE), England’s health technology assessment body, advocates a HbA1c of 48mmol/mol or lower before conception.
NICE also advises that women should not try to conceive if their HbA1c is above 86mmol/mol
National Institute for Health and Care Excellence (NICE). NICE guideline [NG3]. Diabetes in pregnancy: management from preconception to the post-natal period. Available at: https://www.nice.org.uk/guidance/ng3 (accessed September 2017)
Sugar levels during pregnancy via diabetic testing
The desired targets for blood glucose levels should be:
Fasting: 5–7mmol/mol;
Pre-meal: 4–7mmol/mol;
1 hour post-prandial <7.8mmol/mol;
OR
2 hours post-prandial <6.4mmol/mol.
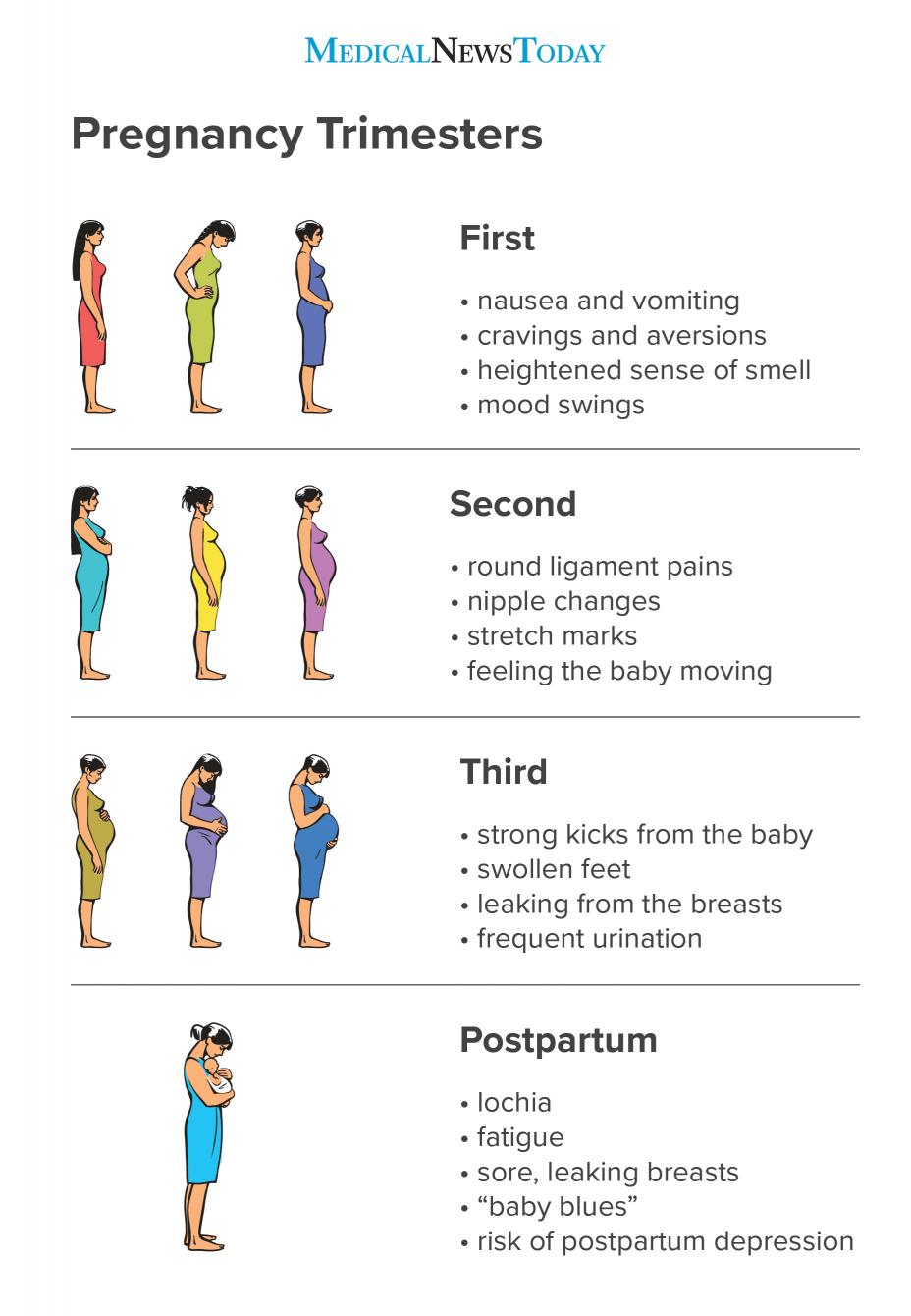
Symptoms of Pregnancy
First trimester
Missing a period
Nausea and vomiting:
Eat small and frequent meals (four to six daily) to maintain blood sugar levels — do not wait until your stomach feels empty
For nausea in the mornings, keep sweet biscuits by your bedside to eat when you first wake and after eating one or two, rest for about 20 minutes before getting up
Eat a diet high in carbohydrates and proteins and low in fat
Avoid spicy foods
Drink plenty of water and fruit juices, but avoid alcohol and large quantities of tea, coffee or milk
Suck barley sugar, boiled sweets or peppermints when travelling
If nausea is worse late in the day, prepare the main meal in the morning
Ask someone to take over chores that heighten nausea, such as cooking or feeding the dog or cat
Some women find that drinking ginger or peppermint tea helps
Balance and dizziness -beware if develop preeclampsia
Otosclerosis – condition in which there’s abnormal bone growth inside the ear (pregnancy does not cause this condition but rather makes the symptoms get worse and progress more rapidly)
Leg cramps especially at night – regular stretching, cold massaging, drink plenty of water, hot showers and movement will help.
Baby’s size and position might make it hard for you to get comfortable
Might be tired of pregnancy and eager to move on to the next stage
Braxton Hicks contractions
Backaches- due to weight of baby and hormones cause muscle tissue to relax-do pregnancy advised regular exercise and stretch afterward. Wear low-heeled — but not flat — shoes with good arch support. – talk to pharmacist for treatments- (back ache tips)
Chorionic villus sampling (This test is usually done around the 11th week of pregnancy and involves removing a tiny piece of the placenta for evaluation)
Amniocentesis (This test is usually done around the 16th week of pregnancy and involves taking a sample of the fluid that surrounds the fetus) testing for genetic tests i.e Tay-Sachs disease and other lysosomal storage diseases disorders
Group B strep -type of bacteria that can live in your vagina or rectum. It can cause a serious infection for your baby if there is exposure during birth. If you test positive for group B strep, your health care provider will recommend antibiotics while you’re in labour.
The British Thyroid Foundation recommend that once aware of the pregnancy, patients should increase their levothyroxine dose by 25–50 micrograms immediately and arrange for a TSH level to be taken.
TSH levels should be monitored every 4–6 weeks during the pregnancy, with the aim of achieving a TSH level of <2.5mU/L in the first trimester and <3.0mU/L in the second and third trimesters.
Patients’ TSH level will need to be checked again a few weeks after birth; most patients are able to return to their previous optimal dose.
Patients wishing to breastfeed should be supported in doing so and should be informed that levothyroxine is safe to be taken when breastfeeding.
Discharge typically continues for four to six weeks after childbirth, a time known as the postpartum period or puerperium.
One may bleed heavily for the first three to ten postpartum days, after which the bleeding should taper off, turning from red to pink, then brown, and finally to a yellowish white.
Lochia should stop sometime between four and six weeks
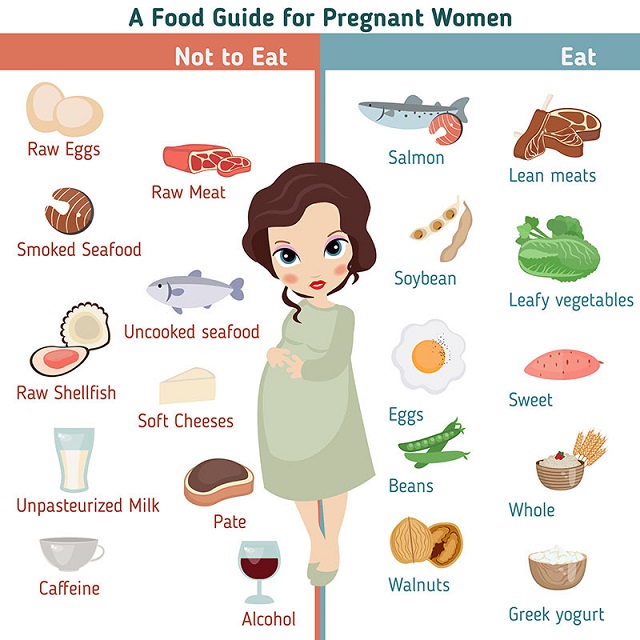
Most foods and drinks are safe to have during pregnancy, but there are some things you should be careful with or avoid.
Too much caffeine can lead to smaller babies who may have health problems later and/or increasing the risk of miscarriage (always check the amount of caffeine content one has from their coffees maker/supplier as the content can vary or look the coffee makers/suppliers website if applicable).
Try and do your best to avoid high content vitamin A products.
Women should not exceed 10,000IU of vitamin A, either before becoming pregnant or at any time during pregnancy as per the guidelines from the National Institute for Health and Care Excellence, England’s health technology assessment body.
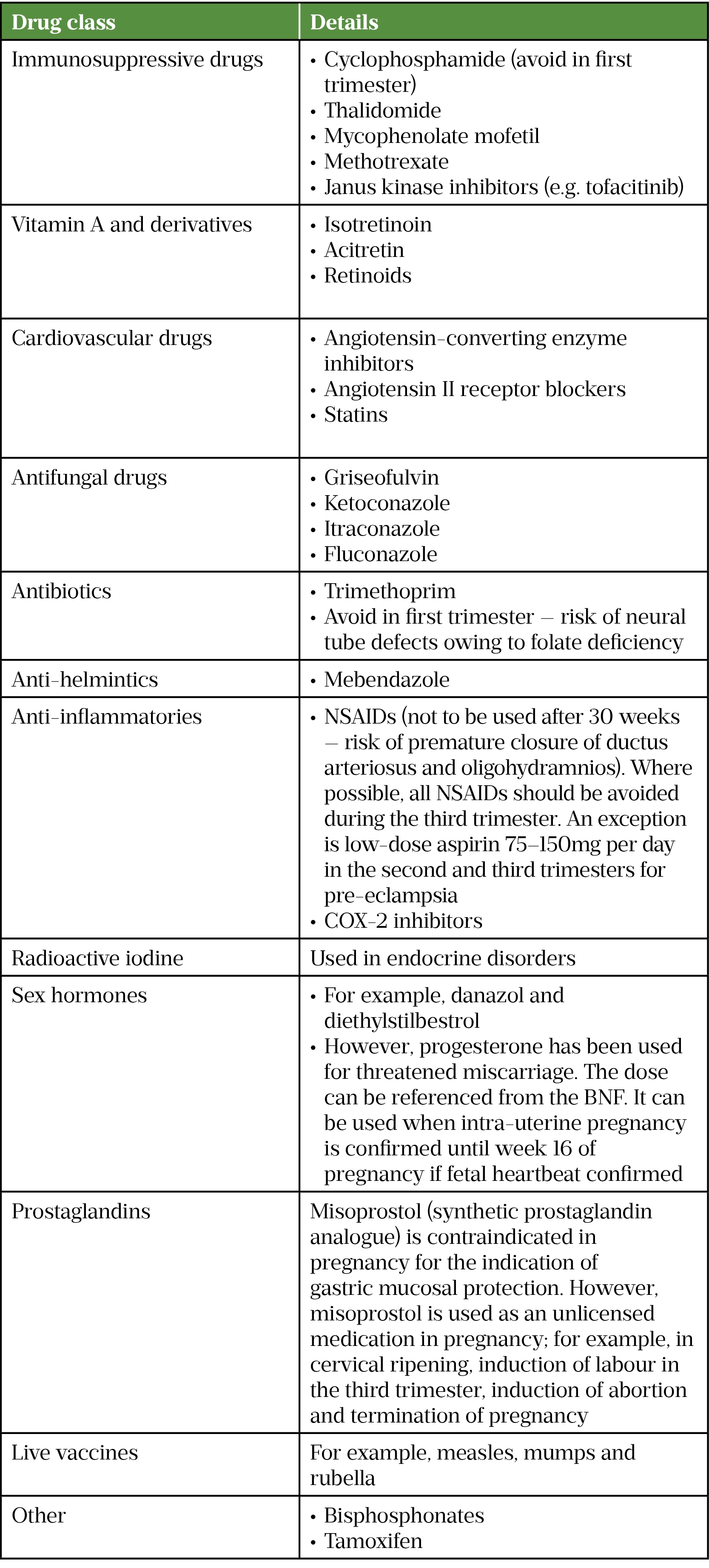
Drugs that are absolutely contraindicated in pregnancy:
Drugs that are absolutely contraindicated in pregnancy
NSAIDs: non-steroidal anti-inflammatory drugs
Most drugs with a molecular weight of less than 1,500 Da can cross the placenta and potentially affect a foetus.
Chatsis V, Frey N. Misoprostol for Cervical Ripening and Induction of Labour: A review of Clinical Effectiveness, CostEffectiveness and Guidelines. CADTH. 2018.https://www.ncbi.nlm.nih.gov/books/ NBK538944/pdf/Bookshelf_NBK538944.
pdf (accessed Jul 2022)
Drugs that are relatively contraindicated in pregnancy:
Other drugs with proven teratogenic effects in humans that are advised to be avoided during pregnancy include:
Tetracyclines (e.g. tetracycline, doxycycline, oxytetracycline). All tetracyclines are contraindicated in the second and third trimesters. These drugs can cause discolouration of deciduous teeth and may have transient effects on foetal bone growth. Tetracyclines may also exacerbate fatty liver of pregnancy. In animal studies, effects on skeletal development have been documented in the first trimester.
Quinolones: Quinolones have been shown to cause arthropathy during neonatal exposure in animal studies.
Chloramphenicol (oral and injection). Owing to the risk of serious haematological side effects, systemic use of chloramphenicol is reserved for the management of life-threatening infections. There are concerns that use near term may be associated with a risk of neonatal ‘grey baby syndrome’, in which the baby has a life-threatening reaction to chloramphenicol, one sign of which is an ashen grey colour of the skin; however, there are no well-documented cases of this occurring. The available data do not indicate that use of ocular chloramphenicol (eye drops) is associated with an increased incidence of congenital malformations; however, other outcomes have not been sufficiently studied to exclude a risk.
Nitrofurantoin (avoid near term). There is a risk of causing haemolytic anaemia in newborns when used near term.
Terbinafine (antifungal). Although the animal reproduction data are encouraging, the lack of human pregnancy experience does not allow a full assessment of the foetal risk from terbinafine. If possible, it would be safer to wait to start treatment until after a pregnancy has completed.
Beta blockers (avoid the use of atenolol in first trimester)
Minoxidil
Diuretics (but appropriate to be used in treatment of pulmonary oedema)
Spironolactone (feminisation has been observed in male rat foetuses)
Endocrine drugs:
Octreotide
Chlorpropamide
If the benefit clearly outweighs the risk (i.e. in life-threatening disease), some ‘relatively contraindicated’ drugs can be used in pregnancy under specialist advice.
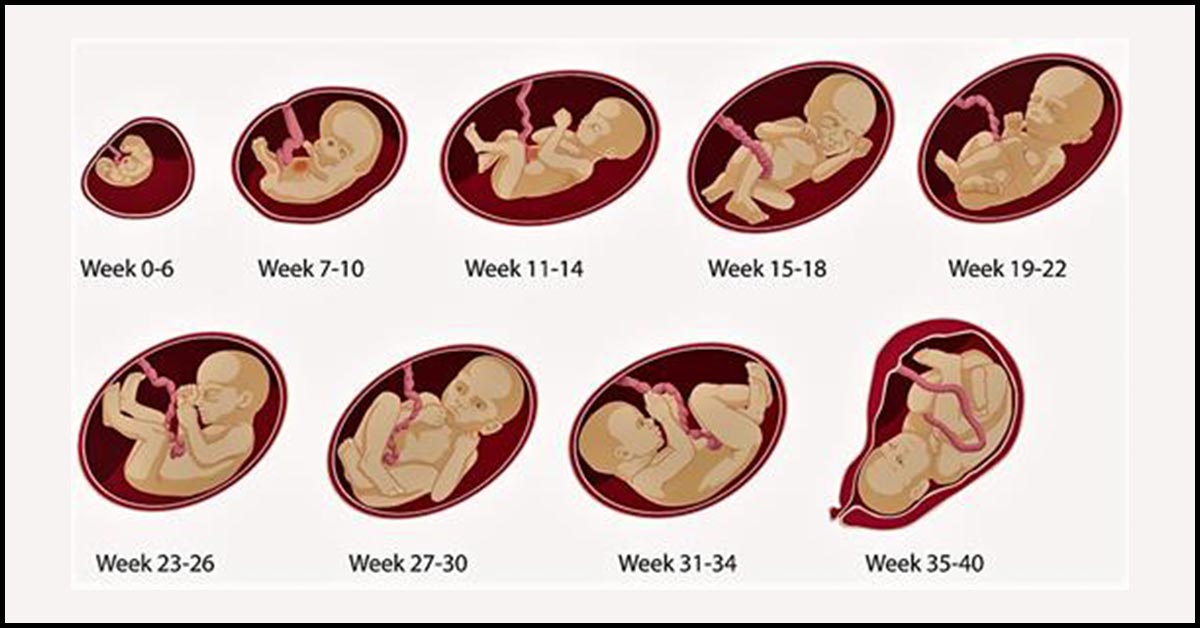
If possible, all drugs should be avoided during the first trimester, which is the period of greatest susceptibility to teratogenic effects. The main risk is structural defects, because the major structures (e.g. brain, spinal cord, arms and legs) and organs are developing at this time;
Only use a medicine when it is absolutely essential;
Use the lowest effective dose for the shortest required duration;
Consider non-pharmacological treatments (e.g. acupressure wrist bands for morning sickness);
Drugs that have been extensively used in pregnancy and are usually safe should be prescribed in preference to new or untried drugs;
Avoid polypharmacy — teratogenicity of a medicine may be enhanced by co-administration of a second medicine or more;
Nelson-Piercy C. Appendix A.1: Prescribing in pregnancy. In: Handbook of Obstetric Medicines. Boca Raton, Florida: : CRC Press 2020. 344–346.
Briggs G, Freeman R, Yaffe S. Drugs in Pregnancy & Lactation:
A Reference Guide to Fetal and Neonatal Risk (12th edn).
Gomes J do A, Olstad EW, Kowalski TW, et al. Genetic Susceptibility to Drug Teratogenicity: A Systematic Literature Review. Front. Genet. 2021;12. doi:10.3389/fgene.2021.645555
Nelson-Piercy C. Appendix A.1: Prescribing in pregnancy. In: Handbook of Obstetric Medicines. Boca Raton, Florida: : CRC Press 2020. 344–346.
Reducing the Risk of Thrombosis and Embolism during Pregnancy and the Puerperium (Green-top Guideline No. 37a). Royal College of Obstetricians and Gynaecologists. 2015.www.rcog.org.uk/globalassets
Pinheiro EA, Stika CS. Drugs in pregnancy: Pharmacologic and physiologic changes that affect clinical care. Seminars in Perinatology. 2020;44:151221. doi:10.1016/j.semperi.2020.151221
Safety review of epilepsy medicines in pregnancy – women who may become pregnant urged to discuss treatment options with their doctor. Medicines and Healthcare products Regulatory Agency. 2021.
Complications /Information to beware of/General tips:
Pregnant females need to be careful when catching infections (infections can be contagious at certain course/point of disease), always talk to a health medical professional if unsure).
One is most prone to complications in the first 3 months of pregnancy as this can lead to miscarriage, premature babies and/or medical conditions passed on to the their baby.
Please see the individual conditions and before having any medication always check with a medical professional to see if its suitable.
Vaginal bleeding (varies from light brown spotting to bright red heavy bleeding or passing blood clots. Bleeding may occur continuously or intermittently over several days)?
Pain or cramping in the lower abdomen?
Discharge of fluid from the vagina (waters may break in a late miscarriage)?
Discharge of tissue from the vagina?
Loss of pregnancy symptoms (e.g. nausea and breast tenderness), in particular if a woman was experiencing strong pregnancy symptoms that abruptly reduce or stop before 12 weeks of pregnancy?
Women can be fertile in the month after a miscarriage, so be cautious/use contraception if another pregnancy is not wanted so soon after a miscarriage
Speak to your Medical Doctor or Midwife to consider:
Risk factors and potential modifying steps that can be taken to reduce risk of future miscarriage:
Eating a healthy, balanced diet, limiting caffeine intake, losing weight before pregnancy.
Avoiding certain foods, such as raw or undercooked meat (which can cause toxoplasmosis), liver and other food products containing vitamin A; meat and vegetarian/vegan patés (which can cause listeriosis); and unpasteurised milk or dairy products (which can cause food poisoning from toxoplasmosis, listeriosis and campylobacter);
Abstaining from drinking alcohol, smoking or using illegal drugs can all reduce the risk of miscarriage and may also lead to the baby having a conditions such as: Sporadic porencephaly.
Make sure your vaccinations are up to date particularly if contracting rubella.
If awaiting investigations following a recurrent miscarriage.
The Pharmaceutical Journal, PJ, May 2022,
Vol 308, No 7961;308(7961)::
DOI:10.1211/PJ.2022.1.144175
Other points to when taking medication and lifestyle treatments in pregnancy:
Some over-the-counter, herbal and vitamin products should be avoided in pregnancy because they may contain ingredients or quantities of ingredients that can cause harm to the foetus;
Medicines given shortly before term or during labour can have adverse effects on labour or on the baby after delivery (e.g. withdrawal effects from opioids);
Alcohol, tobacco and other recreational substances should be avoided during pregnancy.
Counselling services should be considered
Advice on nicotine replacement therapy or non-pharmaceutical therapy when appropriate;
Drinking alcohol, especially in the first three months of pregnancy, increases the risk of miscarriage, premature birth and intrauterine growth restriction.
Drinking after the first trimester affects the baby post-natally.
Drinking heavily (more than six drinks per day) throughout pregnancy can cause the baby to develop foetal alcohol syndrome:
Symptoms of baby include:
Small head
Flat face
Small eye opening
Epicanthal folds (skin fold of the upper eyelid covering the inner corner of the eye)
Short nose
Low nasal bridge
Smooth Philtrum (Flat skin surface, with no ridge formation in the central region of the upper lip between the nasal base and upper vermilion border)
Thin upper lip
Underdeveloped jaw
Genital malformations
Heart (cardiac) defects
Infants often experience alcohol addiction withdrawal symptoms , this may include tremors and/or convulsions, irritability, increased muscle tone, muscle and/or whole body spasms, increased respiratory rate, abdominal swelling (distention) and/or vomiting
Smoking during pregnancy can lead to increased spontaneous abortion, preterm birth, perinatal mortality, infants with low birth weight and stillbirths.
Neonatal exposure is associated with sudden infant death syndrome, asthma, respiratory infections and attention deficit disorder;
Consider maternal contraindications and precautions when advising on a drug in pregnancy, (e.g. avoid recommending labetalol for hypertension in an asthmatic patient);
Closely monitor drugs that have a narrow therapeutic index during pregnancy;
Vaccines made with a live virus (e.g. rubella and varicella vaccines) are not given to women who are, or may be, pregnant;
All women should take folate supplements from the time pregnancy is planned and for the first 12 weeks of pregnancy to reduce the risks of neural tube defects (NTD) in the foetus. A higher daily dose (5mg daily) is recommended for women at a high risk of conceiving a child with NTD, including women who have previously had an infant with NTD, are receiving antiepileptic treatments, or have diabetes or sickle cell disease;
In women diagnosed with hyperemesis gravidarum 9severe and/or prolonged vomiting) a high dose of folic acid (5mg daily) is sometimes used, because vomiting affects the oral absorption of this drug
Consider different routes of administration for drugs used to treat pregnancy complications, such as administering medicines by buccal or rectal route in conditions such as hyperemesis gravidarum;
Venous thromboembolism risk increases with pregnancy because of changes in homeostasis and raised circulating blood volume. The risk is also increased in the presence of pre-existing risk factors, such as clotting disorders, obesity, a positive family history and smoking;
Please talk to your healthcare professional (i.e. Medical Doctor/Pharmacist) for further advice
Detailed Information
Please copy and paste any key words from the title: Pregnancy Symptoms in the following respective 'Medtick References and/or Sources' to find out more about the disease (this also may include diagnosis tests and generic medical treatments).
The Pharmaceutical Journal covers analysis, features, opinion, learning and careers articles, providing insight and knowledge about drugs, pharmacy practice, medicines use and healthcare policy in the context of the pharmacy profession and pharmaceutical science.
Health and fitness news. Recipes, Natural Remedies
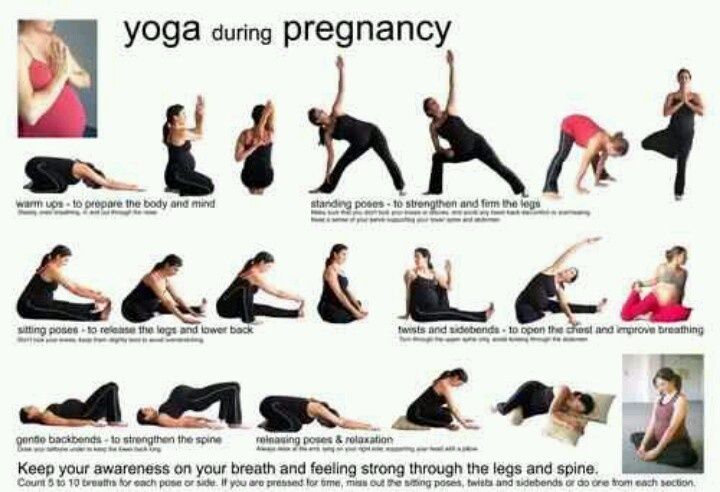
Diet, Exercise and Body Manipulations
Consider a Mediterranean diet (a high intake of fruits, vegetables, whole grains, beans, nuts, and seeds, as well as a lower intake of red meat and dairy), but still be aware of food to avoid in pregnancy especially in conditions:
It may also give better outcomes of higher prevalence of vaginal delivery and a greater prevalence of exclusive breastfeeding for ≥ 16 weeks postpartum.