A condition where bones becomes weak and brittle (thin) and of low bone density (thickness) causing joint pain and difficulty standing up (because legs and hips too weak) or sitting up straight (because spine bone is too weak).
The World Health Organization defines osteoporosis as a “progressive systematic skeletal disease characterised by low bone mass and micro-architectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture”.
It is a result of imbalances between new bone formation and old bone resorption.
In bone resorption, osteoclasts break down bone tissues and release certain minerals that transfer calcium from bone to blood.
Osteoclasts work at a faster rate (and are more active just after menopause) than osteoblasts, the rate of bone loss may outpace the rate of bone production. During these periods new bone is formed but is more prone to fracture as the bone is less densely mineralised, collagen has not matured and reabsorption is not complete.
With osteoporosis, the body may fail to form new bone or too much of the old bone is absorbed.
It is also possible for both events to occur.
Hormones and vitamins that help in the formation and remodelling of bone
Many additional systemic hormones and growth factors influence the generation, function and apoptosis of bone cells. These include growth hormones, glucocorticoid steroids, thyroid hormones and sex hormones (see Table 1).
Table 1. Regulators of bone cells and calcium homeostasis
Hormone
Effect
Parathyroid hormone (PTH)
Increases calcium absorption in the gut;
Increases bone resorption leading to release of calcium;
Increases calcium resorption and phosphate excretion in the kidneys;
Increases hydroxylation of vitamin D precursors (which aid calcium absorption in the gut).
Vitamin D
Increases calcium and phosphate absorption in the gut, thereby promoting bone mineralisation.
Sex hormones
Oestrogen or androgen deficiency accelerates the remodelling rate causing a loss of bone.
Growth hormones
Enhances collagen and non-collagen protein synthesis.
Glucocorticoids
Levels above the physiological norm reduces bone growth and leads to glucocorticoid-induced osteoporosis.
Thyroxine
Thyroid hormones stimulate both bone resorption and formation.
National Institute for Health and Clinical Excellence. Osteoporosis: assessing the risk of fragility fracture. August 2012.
Whyte MP. The long and short of bone therapy. New England Journal of Medicine 2006; 354:860-8636.
Copeland C, Worsley A. Osteoporosis features of disease and diagnosis. Pharm J 2009;1:211-2157.
It develops slowly over a period of years and show very little symptoms
One can lose height.
Diagnosis Tests
Work out if you’re at risk of developing osteoporosis and breaking a bone in the next 10 years.
The self-assessment tool gives a 10-year probability of a fracture in the spine, hip, shoulder or wrist for people aged between 40 and 90.
Estimating your fracture risk could be the first step to getting early treatment to strengthen your bones and reduce your fracture risk.
Treatment can cut your chances of falling and fracturing a bone. It’s never too late to start treatment.
Osteoporosis is usually diagnosed with a bone density scan (called a DEXA or DXA scan).
However, low bone density is not a perfect measure of fracture risk and needs to be considered alongside other risks, such as age, gender, general health and genes.
The FRAX tool, which can be done without a DEXA score, can be a prompt for further discussion about your bone health with your GP to see if a DXA scan is necessary to estimate your risk of future fracture.
NHS
If ones Bone Mineral Density (BMD) T- score is:
Equal or greater than one then one has a normal bone density
If between -1.0 and-2.5 then one has osteopenia (weak bones than normals but not enough to break)
If equal or less than -2.5 then one has osteoporosis.
Bone mineral density scale
Category
Description
T-score
Normal
A value of BMD within 1 standard deviation of the young adult reference mean
≥ -1
Low bone mass (osteopenia)
A value of BMD more than 1 standard deviation below the young adult reference mean but less than 2.5 standard deviations below this mean
< -1 and >-2.5
Osteoporosis
A value of BMD 2.5 standard deviations or more below the young adult reference mean
≤ -2.5
Severe osteoporosis
A value of BMD 4 standard deviations or more below the young adult reference mean
≤ -4
National Osteoporosis guideline Group, Osteoporosis: Clinical guideline for prevention and treatment. March 2014. www.shef.ac.uk/NOGG/NOGG_Executive_Summary.pdf (Accessed 28 March 2014)
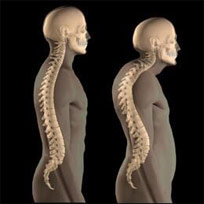
Dowager’s hump or hyperkyphosis is an excessive curvature of the spine. Usually, this occurs in the thoracic or chest curve of the spinal column (appears like a hump on the top ofthe back forcing the neck forward)
Lack of oestrogen in body, i.e. during and after menopause, early menopause before 45 years, hysterectomy (when ovaries removed)
Period absent is greater than six months.
Previous fracture or history of parent hip fracture:
Any previous vertebral fracture (even those detected via radiographic imaging alone) and hip fractures, including the history of a parent with a hip fracture
Pain during movement which goes away at rest (there is normally no pain unless bone is broken)?
Morning body/joint stiffness and goes away quickly (within 30 minutes)?
One side mainly affected i.e. knee, hip?
Hand terminal joints (higher end of fingers) affected not wrist (5- 10 minutes of pain)?
Brittle, soft weak bones, dental problems and/or prone to fractures or curved/bone legs and/or curved spine?
Lower back pain and/or pelvic pain?
Stooping (not appear to stand up straight)?
Loss of height?
Complications /Information to beware of/General tips:
If one is regularly coughing and/or is having breathing difficulties and it hurts their ribs, and/or short of breath, please see your Medical Doctor for a further examination.
Make sure one has adequate Calcium and Vitamin D (have a blood test) and the medical professional will tell you how often and how much to take.
Have regular check ups imaging check ups should be repeated every two years, more often if treatment not helping.
Expert Exercise tips
In patients with osteoporosis, high-impact activities such as jumping; repetitive impact activities such as running or jogging; and bending and twisting activities such as touching one’s toes, golf, tennis, and bowling aren’t recommended because they increase the risk for fracture.
Even yoga poses should be discussed, because some may increase the risk for compression fractures of the vertebrae in the spine.
Strength and resistance training are generally believed to be good for bones.
Strength training involves activities that build muscle strength and mass. Resistance training builds muscle strength, mass, and endurance by making muscles work against some form of resistance. Such activities include weight training with free weights or weight machines, use of resistance bands, and use of one’s own body to strengthen major muscle groups (such as through push-ups, squats, lunges, and gluteus maximus extension).
Some amount of weight-bearing aerobic training is also recommended, including walking, low-impact aerobics, the elliptical, and stair-climbing.
Non–weight-bearing activities, such as swimming and cycling, typically don’t contribute to improving bone density.
In older individuals with osteoporosis, agility exercises are particularly useful to reduce the fall risk (Liu-Ambrose et al; Carter et al). These can be structured to improve hand-eye coordination, foot-eye coordination, static and dynamic balance, and reaction time. Agility exercises with resistance training help improve bone density in older women.
An optimal exercise regimen includes a combination of strength and resistance training; weight-bearing aerobic training; and exercises that build flexibility, stability, and balance.
A doctor, physical therapist, or trainer with expertise in the right combination of exercises should be consulted to ensure optimal effects on bone and general health.
In those at risk for overexercising to the point that they start to lose weight or lose their periods, and certainly in all women with disordered eating patterns, a dietitian should be part of the decision team to ensure that energy balance is maintained. In this group, particularly in very low-weight women with eating disorders, exercise activity is often limited until they reach a healthier weight, and ideally after their menses resume.
Chief, Division of Pediatric Endocrinology, Mass General Hospital for Children; Associate Director, Harvard Catalyst Translation and Clinical Research Center; Director, Pediatric Endocrine-Sports Endocrine-Neuroendocrine Lab; Professor, Department of Pediatrics, Harvard Medical School, Boston, Massachusetts
Disclosure: Madhusmita Misra, MD, MPH, has disclosed the following relevant financial relationships: Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AbbVie; Sanofi; Ipsen
Please talk to your healthcare professional (i.e. Medical Doctor/Pharmacist) for further advice
Detailed Information
Please copy and paste any key words from the title: Osteoporosis in the following respective 'Medtick References and/or Sources' to find out more about the disease (this also may include diagnosis tests and generic medical treatments).
The Pharmaceutical Journal covers analysis, features, opinion, learning and careers articles, providing insight and knowledge about drugs, pharmacy practice, medicines use and healthcare policy in the context of the pharmacy profession and pharmaceutical science.
In patients with osteoporosis, high-impact activities such as jumping; repetitive impact activities such as running or jogging; and bending and twisting activities such as touching one’s toes, golf, tennis, and bowling aren’t recommended because they increase the risk for fracture.
Even yoga poses should be discussed, because some may increase the risk for compression fractures of the vertebrae in the spine.
Strength and resistance training are generally believed to be good for bones.
Strength training involves activities that build muscle strength and mass. Resistance training builds muscle strength, mass, and endurance by making muscles work against some form of resistance. Such activities include weight training with free weights or weight machines, use of resistance bands, and use of one’s own body to strengthen major muscle groups (such as through push-ups, squats, lunges, and gluteus maximus extension).
Some amount of weight-bearing aerobic training is also recommended, including walking, low-impact aerobics, the elliptical, and stair-climbing.
Non–weight-bearing activities, such as swimming and cycling, typically don’t contribute to improving bone density.
In older individuals with osteoporosis, agility exercises are particularly useful to reduce the fall risk (Liu-Ambrose et al; Carter et al). These can be structured to improve hand-eye coordination, foot-eye coordination, static and dynamic balance, and reaction time. Agility exercises with resistance training help improve bone density in older women.
An optimal exercise regimen includes a combination of strength and resistance training; weight-bearing aerobic training; and exercises that build flexibility, stability, and balance.
A doctor, physical therapist, or trainer with expertise in the right combination of exercises should be consulted to ensure optimal effects on bone and general health.
In those at risk for overexercising to the point that they start to lose weight or lose their periods, and certainly in all women with disordered eating patterns, a dietitian should be part of the decision team to ensure that energy balance is maintained. In this group, particularly in very low-weight women with eating disorders, exercise activity is often limited until they reach a healthier weight, and ideally after their menses resume.
Chief, Division of Pediatric Endocrinology, Mass General Hospital for Children; Associate Director, Harvard Catalyst Translation and Clinical Research Center; Director, Pediatric Endocrine-Sports Endocrine-Neuroendocrine Lab; Professor, Department of Pediatrics, Harvard Medical School, Boston, Massachusetts
Disclosure: Madhusmita Misra, MD, MPH, has disclosed the following relevant financial relationships: Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AbbVie; Sanofi; Ipsen