Complications /Information to beware of/General tips:
Medical Emergency Condition
And/or do not wait, phone for an ambulance if have or develop:
- Severe dehydration
- Hypothermia
- CNS depression
- Myxoedema crisis (state of decompensated hypothyroidism)
- Altered mental state:
- Patients can be entirely unconscious
- May be roused by stimuli; usually lethargy and drowsiness have been present for many months
- Defective thermoregulation:
- Hypothermia (as low as 23C) or the absence of fever despite infection
- Presence of a precipitating event:
Clinical Pharmacist, CP, 2011;()::DOI:10.1211/PJ.2021.1.65896
Treatment of Myxoedema crisis in hospital
General measures
- Patients with myxoedema coma require admission to an intensive care or high-dependency unit for careful monitoring and treatment.
- Mechanical ventilation will be required if there is significant hypercapnia or hypoxia. Non-invasive ventilation such as continuous positive airway pressure (CPAP) may used.
- Hypovolaemia, hypoglycaemia and electrolyte disturbances should be corrected.
- Cardiovascular status should be carefully monitored:
- ECG monitoring is essential.
- Myocardial infarction should be excluded.
- Blood pressure should be carefully monitored.
- Pressor agents and inotropes should be avoided, as they provoke arrhythmias.
- Hypothermic patients should be warmed slowly without the use of warming blankets, as peripheral vasodilatation may aggravate or induce hypotension.
Specific measures
- As the numbers of patients with myxoedema coma are relatively small, there are few clinical trials regarding the treatment of these patients.
Thyroid replacement therapy
- Immediate intravenous thyroid replacement is mandatory. Gastrointestinal absorption is compromised.
- There is controversy as to whether this should be T4 alone, combined with T3, or T3 alone.
- It is most common in adults to use T4 alone, with an initial loading dose of intravenous T4 of 100-500 micrograms. This is followed by a dose of 75-100 micrograms per day until the patient is able to take oral replacement.
- It may be combined with T3 in younger patients with lower cardiovascular risk.
Antibiotics
- In view of the fact that many patients will have had their condition precipitated by infection, many advocate adding a broad-spectrum antibiotic to the treatment regime.
Corticosteroids
- It should be assumed that all patients have adrenal insufficiency secondary to hypopituitarism until this can be ruled out, and all patients should receive intravenous hydrocortisone at a dose of 100 mg every eight hours until the results of the random cortisol level prior to treatment are available.
Patient
Pregnancy
If one is pregnant and have poorly controlled thyroxine levels once can have increase risk of :
- Pre-eclampsia
- Miscarriage
- Premature birth and birth defects
- Anaemia in mother
- Bleeding after birth
- Problem with baby development
The British Thyroid Foundation recommend that once aware of the pregnancy, patients should increase their levothyroxine dose by 25–50 micrograms immediately and arrange for a TSH level to be taken.
- TSH levels should be monitored every 4–6 weeks during the pregnancy, with the aim of achieving a TSH level of <2.5mU/L in the first trimester and <3.0mU/L in the second and third trimesters.
- Patients’ TSH level will need to be checked again a few weeks after birth; most patients are able to return to their previous optimal dose.
- Patients wishing to breastfeed should be supported in doing so and should be informed that levothyroxine is safe to be taken when breastfeeding.
The Pharmaceutical Journal, PJ, June 2021, Vol 306, No 7950;306(7950)::DOI:10.1211/PJ.2021.1.
88261
This condition can lead to:
This condition has been associated with:
Test for other conditions
If have any of these conditions one should have a thyroid (or need a high level of thyroid medication) test for:
Thyroxine medication
- Always take it on an empty stomach (for better absorption) ideally before breakfast as directed by a medical doctor at the same time each day
- If one misses a dose, do not take double the dose. Please take the dose as soon as one remembers and continue the next dose at its usual time.
- Do not take with Calcium or iron tablets at the same time with thyroxine affects the absorption of thyroxine. Take at least two hours apart.
- Beware of expiry date of medication and store in a cool dry place away from sunlight, not in the bathroom or kitchen.
- Levothyroxine therapy in patients with diabetes mellitus may worsen glycemic control and result in increased antidiabetic agent or insulin requirements.
- Long-term therapy decreases bone mineral density; use lowest dose in postmenopausal women and women using suppressive doses.
- Thyroid hormone increases metabolic clearance of glucocorticoids medication.
- Starting thyroid hormone therapy before initiating glucocorticoid therapy may precipitate an acute adrenal crisis in patients with adrenal insufficiency.
- Treat patients with adrenal insufficiency with replacement glucocorticoids before starting treatment with thyroid hormone.
- Levothyroxine toxicity
- is uncommon and is most likely due to accidental ingestion.
- The onset of signs and symptoms may be delayed 3-10 days, owing to the time of T4 to be metabolized to the more active T3.
- Symptoms may include nervousness, insomnia, tremor, tachycardia, body temperature elevation, and loose stools.
Thyroid testing
- Thyroxine levels should be checked every four to six months by your medical doctor via a blood test and more regularly if poorly controlled. The dose of medication is based upon your test results.
- American Thyroid Association guidelines state the following:
- If levothyroxine dose requirements are much higher than expected, consider evaluating for gastrointestinal disorders, such as Helicobacter pylori–related gastritis, atrophic gastritis, or celiac disease; if such disorders are detected and effectively treated, revaluation of thyroid function and levothyroxine dosage is recommended.
- Initiation or discontinuation of oestrogen and androgens should be followed by reassessment of serum TSH at steady state because such medications may alter the levothyroxine requirement.
- Serum TSH should be reassessed upon initiation of such agents as tyrosine kinase inhibitors that affect thyroxine metabolism and thyroxine or triiodothyronine deiodination.
- Serum TSH monitoring is advisable when such medications as phenobarbital, phenytoin, carbamazepine, rifampin, and sertraline are started.
- When deciding on a starting dose of levothyroxine, the patient’s weight, lean body mass, pregnancy status, aetiology of hypothyroidism, degree of TSH elevation, age, and general clinical context, including the presence of cardiac disease, should be considered. The serum TSH goal appropriate for the clinical situation should also be considered.
- Thyroid hormone therapy should be initiated as an initial full replacement or as partial replacement with gradual increments in the dose titrated upward using serum TSH as the goal.
- Dose adjustments should be made upon significant changes in body weight, with aging, and with pregnancy; TSH assessment should be performed 4-6 weeks after any dosage change.
- Reference ranges of serum TSH levels are higher in older populations (i.e. > 65 years), so higher serum TSH targets may be appropriate.
Please see your Medical Doctor even if display some symptoms as as symptoms can vary from individual to individual
The following raw foods in high consumption can cause slow one thyroid function down (thyroid surgery and/or radiation treatment of thyroid is not affected by these foods):
- African cassava
- Babassu (a palm-tree coconut fruit found in Brazil and Africa)
- Bok choy
- Broccoli
- Broccolini
- Brussels sprouts
- Cabbage
- Canola
- Cauliflower
- Chinese Broccoli
- Collards
- Daikon
- Flax
- Kale
- Kohlrabi
- Millet
- Mustard
- Peaches
- Peanuts
- Pine nuts
- Radishes
- Red Radish
- Rutabaga
- Spinach
- Strawberries
- Sweet potato
- Turnips
- Watercress
Some foods containing flavonoids:
- Berries
- Red wine
- Soy products such as tofu, tempeh, edamame, and soy milk
- Teas, especially green, white, and oolong varieties
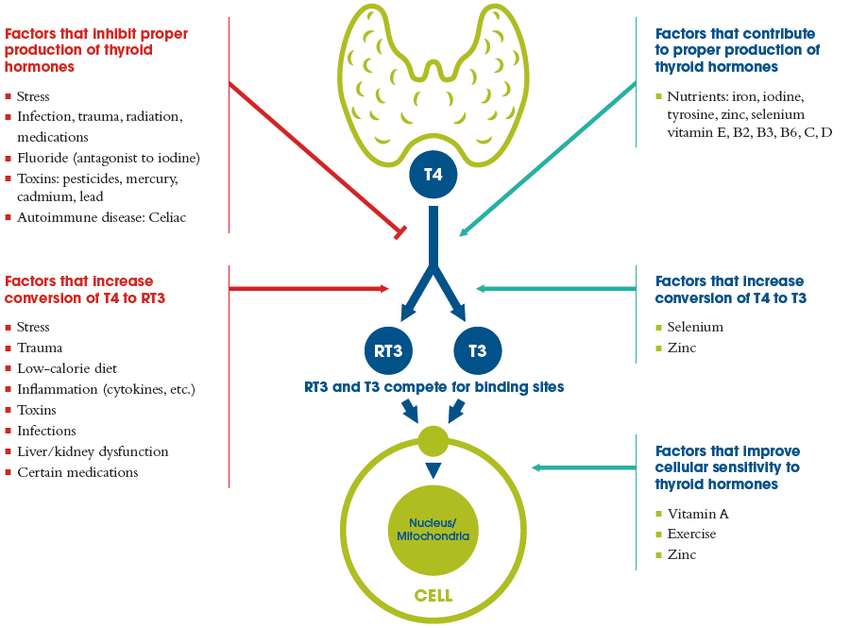
One can increase their intake of iodine and selenium products to increase thyroid function:
- Foods include (iodine rich foods):
- Seaweed
- Kelp
- kombu
- Nori
- Iodized salt
- Foods include (selenium rich foods):
- Brazil nuts
- Fish
- Meat
- Sunflower seeds
- Tofu,
- Baked beans
- Portobello mushrooms
- Whole grain pasta
- Cheese
- Also one should increase their intake of
- Vitamin A
- Vitamin B2
- Vitamin B3
- Vitamin B6
- Vitamin C
- Vitamin D
- Zinc
Please talk to a Dietitian of the above foods if one has a low thyroid function
Do not take iodine vitamin supplements unless a healthcare professional advises otherwise. If one does take such a supplement, one should have regular blood tests and adjust does of any medication for this condition accordingly and also let the healthcare professional know on what does of iodine one takes and for how long.
This condition may have similar symptoms to:
Please talk to your healthcare professional (i.e. Medical Doctor/Pharmacist) for further advice