(Diabetes type 1 mellitus, Insulin-dependent diabetes, juvenile diabetes)
What is it?
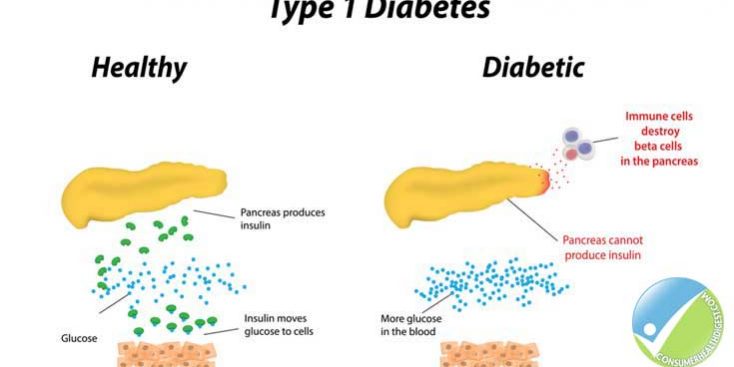
A condition resulting from beta-cell destruction in the pancreas, leading to a severe impairment of insulin secretion and eventual absolute insulin deficiency causing is too much glucose (sugar) in the blood as it does not move to the body organs easily because a lack of insulin.
It is less common than diabetes type 2 and occurs in patients under 40 years and young persons.
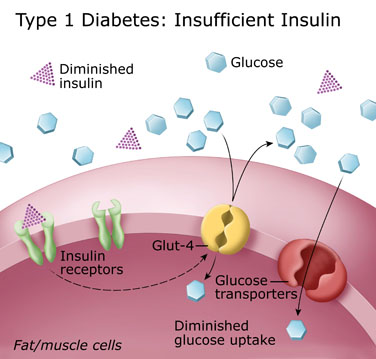
Insulin in required to move glucose from the blood to the cells. It is in the cell when glucose is broken to make energy.
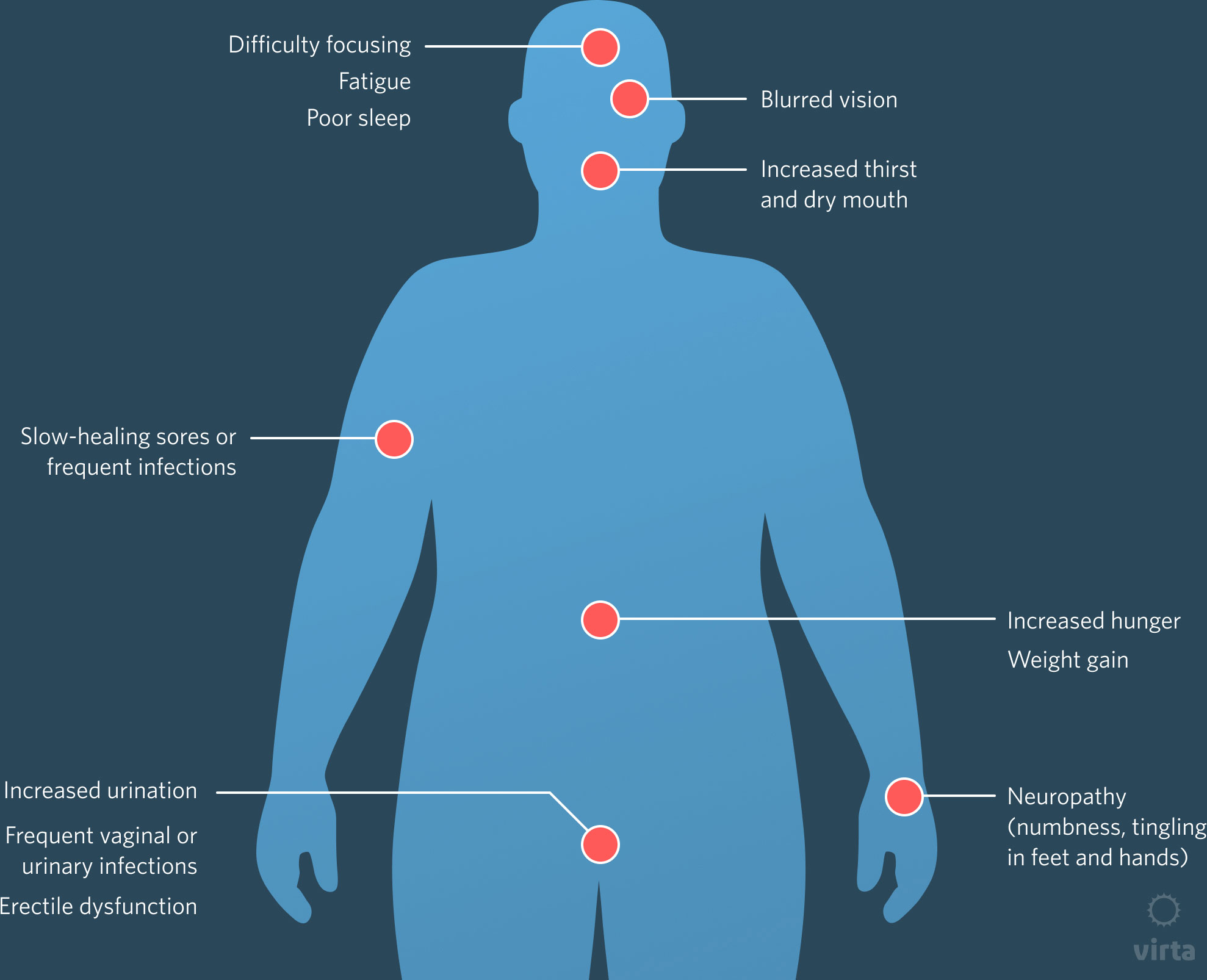
In diabetes type 1 condition, the body produces no insulin and symptoms can be very sudden.
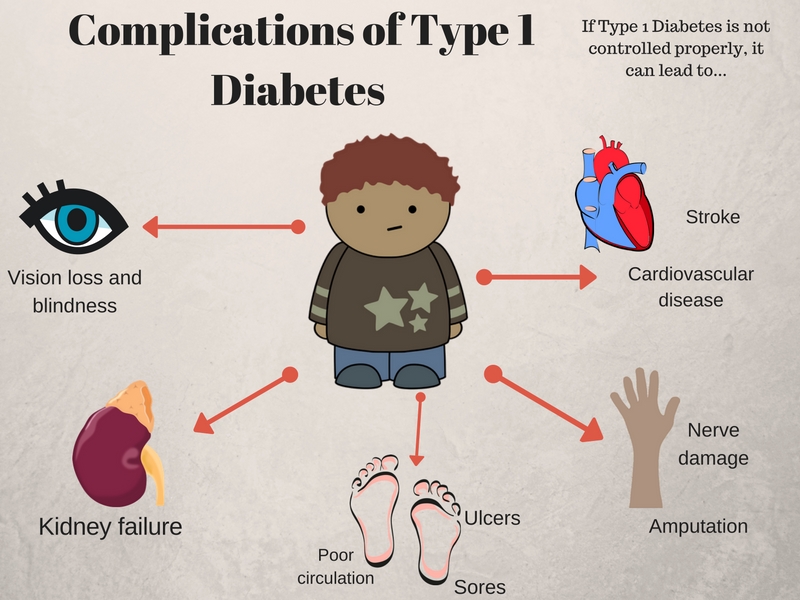
It is important to diagnose diabetes and control it since it can increase the chance of heart conditions, kidney disorders, blindness, nerve disorders, poor circulation causing skin infections, erectile dysfunction and nerve disorders.
Diagnosis of diabetes includes any of the following:
A fasting plasma glucose level ≥ 126 mg/dL (7 mmol/L); fasting is defined as no caloric intake for at least 8 hours
A 2-hour plasma glucose level ≥ 200 mg/dL (11.1 mmol/L) or during a 75-g oral glucose tolerance test
An A1c level ≥ 6.5% (≥ 48 mmol/mol)
A random plasma glucose level ≥ 200 mg/dL (11.1 mmol/L) in a patient with classic symptoms of hyperglycemia (ie, polyuria, polydipsia, polyphagia, weight loss) or hyperglycemic crisis
Measuring concentrations of insulin or C-peptide (a fragment of proinsulin that serves as a marker for insulin secretion) is rarely necessary to diagnose diabetes type 2 or differentiate diabetes 2 from Diabetes type 1. Insulin levels generally are high early in the course of diabetes type 2 and gradually wane over time. A fasting C-peptide level > 1 ng/dL in a patient who has had diabetes for more than 1-2 years is suggestive of diabetes type 2 (ie, residual beta-cell function).
American Diabetes Association (ADA)
Poor sugar control
‘Please see your medical doctor even if display some symptoms as as symptoms can vary from individual to individual’
Please beware of hypoglycaemia (poorly controlled diabetes) when having low sugar levels, poor controlled diet and poor control and use of diabetic medication
Glucose testing
Patients who have confirmed diabetes should have a glucose test annually by a medical doctor, more often if not controlled.
Maybe caused by our own immune system attacking the beta cells in the pancreas [(type 1A), (type 1B) reactions and/or cytotoxic CD8+ T cells attacking the beta- cells).
Maybe caused by our own immune system attacking the beta cells in the pancreas [(type 1A), (type 1B) reactions and/or cytotoxic CD8+ T cells attacking the beta- cells).
Eating too much (one should have regular size meals at same time each day).
DIABETES TYPE 2
What is it?
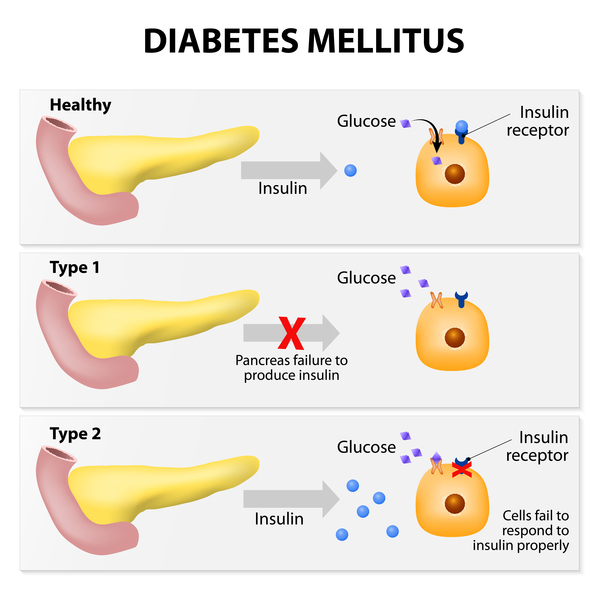
This type of diabetes is when one has too much glucose (sugar) in blood.
This is the most common form and is usually diagnosed to patients over 40 years. However it can occur in persons younger due to being overweight and obese.
Insulin is needed to move glucose into cells of the body; cells break down glucose and use it for energy.
In diabetes type-2 the body does not produce enough insulin or does not use insulin correctly even though adequate amounts are produced when having condition.
This condition develops more slowly than diabetes type 1.
One may experience very mild symptoms (initially) and patients do not notice the condition since it is not having a major impact on their lives.
It is important to diagnose diabetes and control it (since it is a progressive disease) and can increase the chance of heart conditions, kidney disorders, blindness, nerve disorders, poor circulation causing skin infections, erectile dysfunction and nerve disorders.
A patient’s diabetes result after doing a glucose test of HbA 1c 53mmol/l (HbA 1c(%) 7.0mmol/l) or greater could indicate diabetes.
Glucose Testing
Testing should be considered in overweight or obese adults who have one or more of the following risk factors:
Other clinical conditions associated with insulin resistance (eg, severe obesity, acanthosis nigricans)
Testing should begin at age 45 years.
Testing for prediabetes and/or diabetes type 2 in asymptomatic patients should be considered in adults of any age who are overweight or obese and who have one or more additional risk factors for diabetes.
Among Asian, a BMI ≥ 23 kg/m2 is the threshold for all other persons, a BMI ≥ 25, kg/m2 is the threshold.
American Diabetes Association (ADA)
Diagnosis of diabetes includes any of the following:
A fasting plasma glucose level ≥ 126 mg/dL (7 mmol/L); fasting is defined as no caloric intake for at least 8 hours
A 2-hour plasma glucose level ≥ 200 mg/dL (11.1 mmol/L) or during a 75-g oral glucose tolerance test
An HBA1c level ≥ 6.5% (≥ 48 mmol/mol) on two separate occasions (usually taken two to four weeks apart).
A random plasma glucose level ≥ 200 mg/dL (11.1 mmol/L) in a patient with classic symptoms of hyperglycemia (ie, polyuria, polydipsia, polyphagia, weight loss) or hyperglycemic crisis
Measuring concentrations of insulin or C-peptide (a fragment of proinsulin that serves as a marker for insulin secretion) is rarely necessary to diagnose diabetes type 2 or differentiate diabetes 2 from Diabetes type 1. Insulin levels generally are high early in the course of diabetes type 2 and gradually wane over time. A fasting C-peptide level > 1 ng/dL in a patient who has had diabetes for more than 1-2 years is suggestive of diabetes type 2 (ie, residual beta-cell function).
American Diabetes Association (ADA)
National Institute for Health and Care Excellence-recommended treatment targets for people with type 2 diabetes mellitus
HbA1c ≤58.0mmol/mol (7.5%);
Blood pressure <140/80mmHg;
Total cholesterol <5mmol/L and HDL<4mmol/L.
National Institute for Health and Care Excellence. Type 2 diabetes in adults: management. NICE guideline [NG28]. 2019. Available at: https://www.nice.org.uk/guidance/NG28
(accessed September 2019)
Poor sugar control
‘Please see your medical doctor even if display some symptoms as as symptoms can vary from individual to individual’
Please beware of hypoglycaemia (poorly controlled diabetes) when having low sugar levels, poor controlled diet and poor control and use of diabetic medication
Glucose testing
Patients who have confirmed diabetes should have a glucose test annually by a medical doctor, more often if not controlled.
Peripheral vascular disease – blood circulation affecting all major blood vessels outside the heart especially painful cramps and artery damage on legs and increase risk of heart disease as well as taking the body longer to heal.
One should have routine eye tests at least every two years but if one has concerns one should book an eye test at any point
Persons over 40 years should have eye test at least every 2 years and you must tell drivers authority if it affects your driving
General tips
Hot baths and massage
Some diabetics cannot tell if their skin feels hot or cold sensations (peripheral neuropathy) and may burn their skin leading to skin infection and/or a serious muscle breakdown called rhabdomyolysis.
Hot baths can increase blood flow and may reduce blood glucose levels in one’s blood due to an increase in insulin levels produced by ones body.
Massages are fine if one has no poor circulation, it is not fine if one has poorly controlled or advanced diabetes and/or is prone to muscle breakdown this can lead to numbness, heart problems and/or kidney failure as well as a serious muscle breakdown called rhabdomyolysis.
Avoid massaging areas when one has insulin injected as the pressure in the area may influence the way their body absorbs the shot and their alter their intake.
Excessive heat can can cause your heart to beat faster which may be of concern if one has an underlying heart issue/cardiovascular issue.
Foot care Patient Advice (especially diabetics or with poor foot circulation)
Look at feet each day. If you are not able to check if someone else can, particularly if you have reduced sensation in feet.
If you get a cut, bruises, redness, blister bleeding; please see your medical doctor, in the meantime cover it up with a clean dry dressing.
If you have dry skin, use a moisturising cream or oil but do not use between toes (one may have athletes foot or be at risk).
Cut your nails along curvature with toe nail clippers, not straight across. Do not damage your skin.
Wash feet regularly everyday in warm soapy (anti-bacterial soap) and/or salty (antiseptic) water especially between toes and ‘pat dry’ thoroughly.
Try to avoid foot burns:
Check bath temperature with hand before you put your feet in.
Keep your feet away from hot objects e.g. hot water bottles, electric blankets, close to fire, hearers
Avoid slip on shoes
Avoid top flat shoes, pointy shoes (have broad front with room for toes, sandals and flip flops that cause rubbing).
Always feel inside shoes for stones or rough edges before you put them on.
Always wear comfortable low heel shoes/trainers, (heels too low can strain the foot arch, cause sore and cracked heels)
Make sure they fit well (comfortable fastening, liner and buckles to prevent rubbing otherwise can get blisters). Take into account any corns, bunions, awkward shape. (If have no choice, consider specially fitted shoes to take account of bunions, corns deformities)
When buying new shoes, wear your usual socks.
Gradually break in new shoes.
Always wear comfortable socks (not too tight) with footwear. Socks protect you from a rubbing shoe.
Do not walk bare foot anywhere. One may damage their feet.
Rotate ones ankles move feet up and down and do regular feet exercise to improve suppleness and blood circulation.
This condition may show similar symptoms to other types of diabetes and/or other conditions:
Please talk to your healthcare professional (i.e. Medical Doctor/Pharmacist) for further advice
Detailed Information
Please copy and paste any key words from the title: Diabetes in the following respective 'Medtick References and/or Sources' to find out more about the disease (this also may include diagnosis tests and generic medical treatments).
The Pharmaceutical Journal covers analysis, features, opinion, learning and careers articles, providing insight and knowledge about drugs, pharmacy practice, medicines use and healthcare policy in the context of the pharmacy profession and pharmaceutical science.