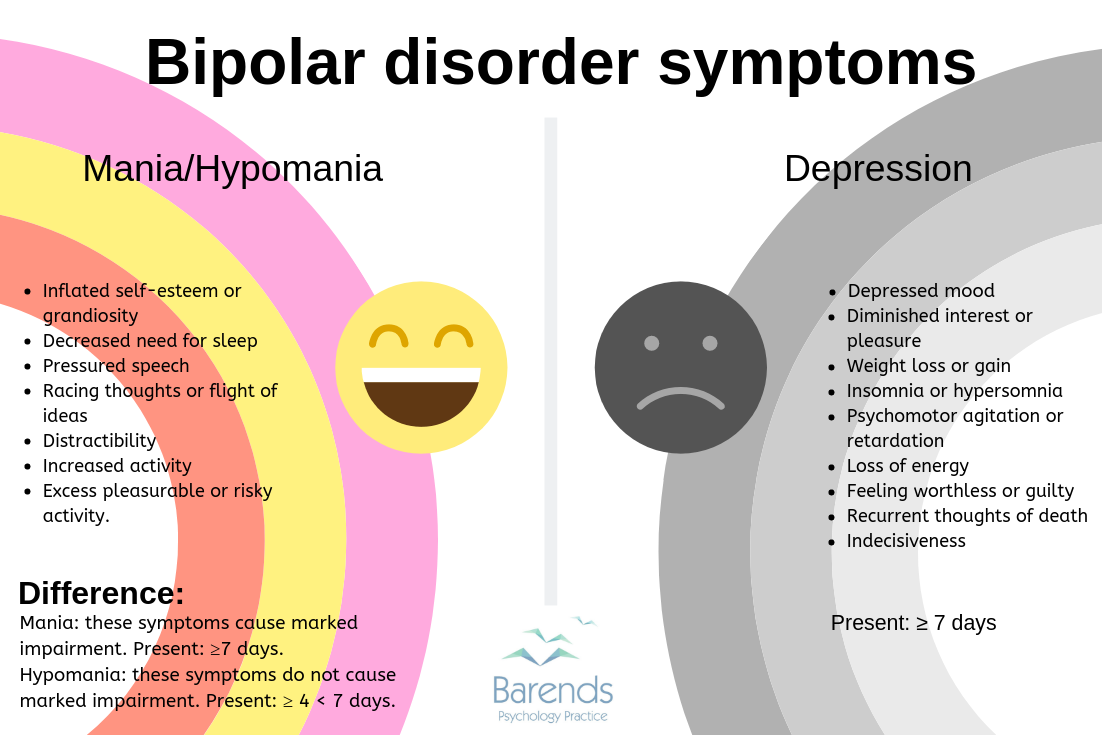
A mental disorder known by wide and/or extreme mood swings from extreme high episodes (mania, manic, sense of euphoria, buzz, full of energy , irritable and anxiety) mood to extreme low mood episodes (depression).
Mild symptoms of mania and those who does not have psychotic symptoms (delusions-false beliefs and hallucinations – false perception i.e. taste and smell things differently and/or hear voices) is known as ‘hypomania’ or a hypomanic episode.
It is also referred as Manic Depressive Illness or Manic Depression.
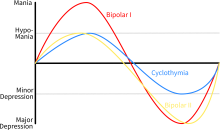
Bipolar mood disorder will continue to evolve, but it is now commonly divided into two subtypes:
Bipolar I disorder is the classic form where a person has had at least one manic episode.
A distinct period of pure manic or mixed episodes lasting for all or most of at least 1 week, nearly every day (or any length if hospitalized) would be diagnosed as bipolar I disorder on the basis of the DSM-5 (diagnosis handbook to diagnose mental disorders).
A manic episode is an abnormally and persistently expansive, elevated, or irritable mood accompanied by at least three other symptoms (four if the primary mood is irritable).
Mixed episodes feature mania intermixed with symptoms of a major depressive episode that cause significant impairment of functioning and/or require hospitalization.
Bipolar II is at least one hypomanic episode and at least one major depressive episode are not better explained by schizoaffective disorder and are not superimposed on schizophrenia, schizophreniform disorder, delusional disorder, or other specified or unspecified schizophrenia spectrum and other psychotic disorder.
In bipolar II disorder, the person has never had a manic episode, but has had at least one hypomanic episode and at least one period of significant depression (with a distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistently increased activity or energy lasting at least 4 consecutive days and present most of the day or nearly every day that does not require hospitalization).
Patients with bipolar II disorder in this hypomanic state can function socially and vocationally, and they can be remarkably efficient and sometimes effective.
Bipolar II disorder had a history of rapid cycling and/or high number of episodes.
It is also found that bipolar II disorder was more likely to be rated chronic fluctuating rather than episodic (discrete periods) throughout its lifetime clinical course.
Bipolar II disorder was associated with later age at first hypomania and treatment, later bipolar presentation, less frequent referral after a single episode, and more episodes before lithium treatment.
The course of bipolar II disorder was typically characterized by early depressive onset and episodes, depressive predominant polarity, and multiple depressive recurrences; hypomania or hypomania-depression cycles were less common at onset or during the early course of bipolar II disorder.
Bipolar II disorder were more likely to be older, women, and married or widowed rather than single. They also found that more patients with bipolar II disorder had first-degree relatives affected by anxiety disorders and major depression.
Researchers no differences in age at onset of depressive episodes and mood disorders, family history of suicide, global functioning, lifetime suicide attempts, and lithium response between patients with bipolar I disorder and those with bipolar II disorder.
Others:
Cyclic manic and depressive symptoms of any duration are typically diagnosed as cyclothymia when the symptoms are not sufficient for a diagnosis of either bipolar I or bipolar II disorder but have occurred for at least a 2-year period with symptom-free intervals of under 2 months.
Major depressive disorder are five or more symptoms, including either depressed mood or loss of interest or pleasure that represent a change from previous functioning and are present during the same 2-week period, contribute to a diagnosis of major depressive disorder in the DSM-5.
Medscape
Further Information
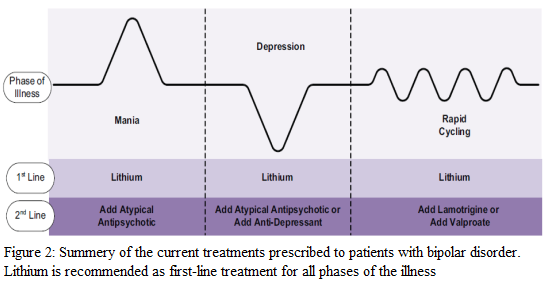
Some persons with bipolar mood disorder switch frequently or rapidly between manic and depressive symptoms, a pattern that is often called “rapid cycling.” If manic and depressive symptoms overlap for a period, it is called a “mixed” episode. During such periods, it may be difficult to tell which mood — depression or mania — is more prominent.
Harvard Health publications
Vulnerability
Vulnerability must be noted. The prevalence of bipolar disorder type 1 is generally equal between men and women; however, several studies have found a higher rate of type 1 among men and type 2 among women.
Medscape
Suicidal attempts are very common in this condition, urgent medical referral and treatment is required
Cause
Chemical imbalances in the brain between nerve transmitters (chemicals that send send signal between nerves and brain and spinal cord i.e. noradrenaline, serotonin and dopamine)
Bipolar disorder, especially type 1, has a major genetic component, with the involvement of the ANK3, CACNA1C, and CLOCK genes.
For medication to cause mania and/or depression the following criteria needs to be met:
DSM-5 criteria for substance/medication-induced mental disorders are:
The disorder is a clinically significant symptomatic presentation of a relevant mental disorder.
Evidence from the history, physical examination, or laboratory findings supports both of the following:
The disorder developed during or within 1 month of a substance intoxication or withdrawal or taking a medication; and
The involved substance/medication is capable of producing the mental disorder.
The disorder is not better explained by an independent mental disorder (ie, one that is not substance- or medication-induced). Such evidence of an independent mental disorder could include:
The disorder preceded the onset of severe intoxication or withdrawal or exposure to the medication; or
The full mental disorder persisted for a substantial period of time (i.e. ≥ 1 month) after the cessation of acute withdrawal or severe intoxication or taking the medication.
The disorder does not occur exclusively during the course of a delirium.
The disorder causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Doing things that often have disastrous consequences – such as spending large sums of money on expensive and sometimes unaffordable items?
Making decisions or saying things that are out of character and that others see as being risky or harmful?
After this phase is over , the person may not believe that they could behave this way and may believe other persons around them are being negative or unhelpful towards them?
Bipolar depression (different from normal depression)- long phase
Distinctly low or irritable mood?
Loss of interest or pleasure in everyday activities?
Eating more or less than normal?
Gaining or losing weight?
Sleeping more or less than normal?
Appearing slowed or agitated about everything?
Fatigue and loss of energy?
Feeling sad, hopeless, worthless, emptiness and/or guilty and/or despair?
Poor concentration and remembering things?
Cannot make a decision?
Self doubt?
Thoughts/thinking of death, suicide attempts or plans?
Complications /Information to beware of/General tips:
This condition is similar to:
Cyclothymia (Persons with this disorder fluctuate between hypomania and mild or moderate depression without ever developing a full manic or depressive episode)
Cyclothymic disorder is a lifelong fluctuating mood disorder on the bipolar spectrum that involves recurrent episodes of hypomanic symptoms and recurrent episodes of depressive symptoms. Importantly, these episodes fall short of meeting the full criteria for hypomanic or manic episodes and major depressive episodes. Thus, cyclothymic disorder is often viewed as a milder form of bipolar disorder in some respects. It has these specific diagnostic criteria
For at least 2 years (at least 1 year in children and adolescents), there have been numerous periods with hypomanic symptoms that do not meet criteria for a hypomanic episode and numerous periods with depressive symptoms that do not meet criteria for a major depressive episode.
During the above 2-year period (1 year in children and adolescents), criterion A symptoms have been present for at least half the time and the individual has not been without the symptoms for more than 2 months at a time.
Criteria for a major depressive, manic, or hypomanic episode have never been met.
The symptoms in criterion A are not better explained by schizoaffective disorder, schizophrenia, delusional disorder, or other specified or unspecified schizophrenia spectrum and other psychotic disorder.
The symptoms are not attributable to the physiological effects of a substance (i.e. a drug of abuse, a medication) or another medical condition (i.e. hyperthyroidism).
The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013
Type of depression that’s related to changes in seasons — SAD begins and ends at about the same times every year.
Persons with mood changes are sensitive to light changes (due to hypothalamus function in the brain):
Less light- lenghthens the sleep -wake cycle leading to depression.
More light- shortens the sleep- wake cycle leading to mania.
Symptoms of depression are more intense symptoms during the winter (peak symptoms usually occur during spring and fall months) and less intense symptoms during the summer sapping your energy and making you feel moody.
The main age of onset for SAD is 18-30 years; SAD is less likely to occur in older adults.
Most individuals who experience SAD are women.
To be diagnosed with SAD, an individual must demonstrate at least two episodes of depressive disturbance in the previous 2 years and seasonal episodes should substantially outnumber nonseasonal episodes.
Symptoms, including hypersomnia (excessive daytime sleepiness), increased appetite, and craving for carbohydrates( sugar). Spring/summer SAD is more frequently associated with insomnia and loss of appetite.
treatment is to increase light exposure in the winter and decrease light exposure in the summer:
Leave bedroom curtain/shutter open (increase morning sun exposure), use sunglasses less, seek the sun , walk during noon in the winter/spring and fall months.
Consider light therapy in winter months only (not spring and falls).
Leave bedroom curtain/shutter closed (reduce morning sun exposure), wear sun glasses and/or wear an eye mask at night in the summer.
Please talk to your healthcare professional (i.e. Medical Doctor/Pharmacist) for further advice
Detailed Information
Please copy and paste any key words from the title: Bipolar Mood Disorder in the following respective 'Medtick References and/or Sources' to find out more about the disease (this also may include diagnosis tests and generic medical treatments).
The Pharmaceutical Journal covers analysis, features, opinion, learning and careers articles, providing insight and knowledge about drugs, pharmacy practice, medicines use and healthcare policy in the context of the pharmacy profession and pharmaceutical science.