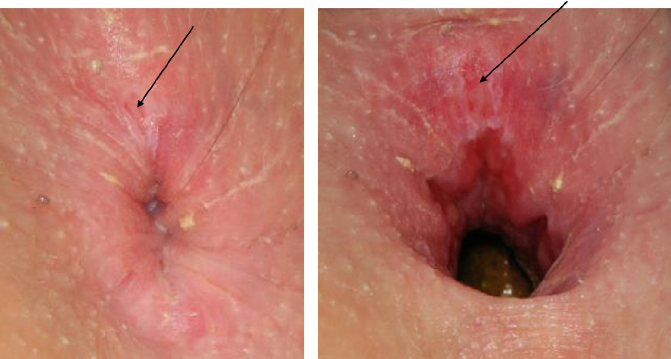
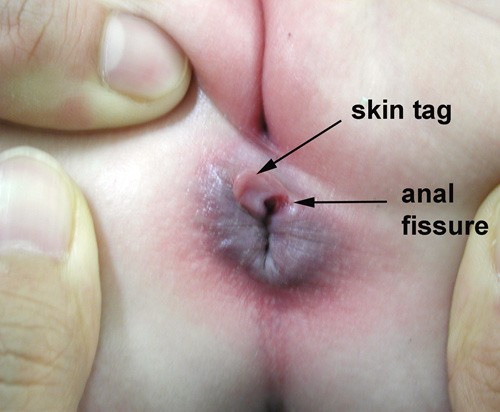
An anal fissure is a tear or open sore (ulcer) that develops in the lining of the anal canal.
In the short term, anal fissures usually involve only the epithelium.
In the long term, they involve the full thickness of the anal mucosa.
Anal fissures develop with equal frequency in both sexes; they tend to occur in younger and middle-aged persons.
Diagnosis Tests
Labatory tests are preformed if one has an underlying condition listed below or if anal fissures are irregular or if located off the midline, ordinary anal fissures are located on the anterior or posterior midline, no laboratory tests are necessary.
These can include:
Erythrocyte sedimentation rate
Biopsy of fissure or lesions (as warranted)
Stool and viral cultures
HIV testing
Medscape
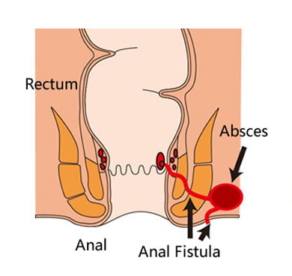
An anal fistula is a small tunnel that develops between the end of the bowel and the skin near the anus (where poo leaves the body). They’re usually the result of an infection near the anus causing a collection of pus (abscess) in the nearby tissue.
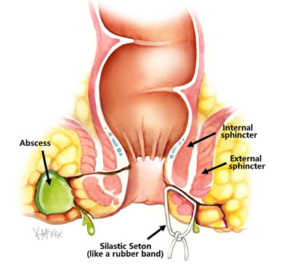
Anal fistulas are classified into four general types:
Intersphincteric: through the dentate line to the anal verge, tracking along the intersphincteric plane, ending in the perianal skin , they are the most common.
An intersphincteric fistula-in-ano is caused by a perianal abscess. In its most common course, it begins at the dentate line, then tracks to the space between the internal and external anal sphincters (the intersphincteric space) via the internal sphincter, and finally terminates in the perineum or perianal skin.
Transsphincteric: through the external sphincter into the ischiorectal fossa, encompassing a portion of the internal and external sphincter, ending in the skin overlying buttocks.
Suprasphincteric: through the anal crypt and encircling the entire sphincter, ending in the ischiorectal fossa.
Extrasphincteric: starting high in the anal canal, encompassing the entire sphincter and ending in the skin overlying the buttocks.
Other possible tracts include high tract to pelvis or lower rectum, high blind tract, or no perineal opening.
Most anal fistulas originate in anal crypts, which become infected, with ensuing abscess formation. When the abscess is opened or when it ruptures, a fistula is formed.
Opened perianal or ischiorectal abscesses, which drain spontaneously through these fistulous tracts.
Sharp pain when you pass stools, often followed by a deep burning pain that may last for a few minutes to last several hours afterwards?
Pain recurs with every bowel movement, and the patient commonly becomes afraid or unwilling to have a bowel movement, leading to a cycle of worsening constipation, harder stools, and more anal pain?
One find passing stools difficult (can be painful) and constipated?
Please talk to your healthcare professional (i.e. Medical Doctor/Pharmacist) for further advice
Detailed Information
Please copy and paste any key words from the title: Anal Tear and/or Fissure and Anal Fistulas in the following respective 'Medtick References and/or Sources' to find out more about the disease (this also may include diagnosis tests and generic medical treatments).
The Pharmaceutical Journal covers analysis, features, opinion, learning and careers articles, providing insight and knowledge about drugs, pharmacy practice, medicines use and healthcare policy in the context of the pharmacy profession and pharmaceutical science.