
(please note that inhalers, creams, scalp applications eyes ears and nose drops and sprays rarely cause side effects since they go directly into the affected area, however if you have used it a long time or have recently started and feel poorly please see the doctor)
Source: Isle of Wight NHS Trust
Please let your medical prescriber know the following when undertaking using an inhaler:
Figures 1–5 provide a summary of the techniques for the commonly used inhaler devices, and common errors with patient technique, that healthcare professionals can use as a guide before training patients.

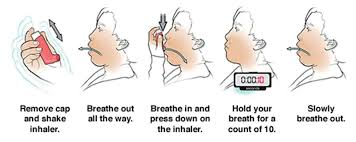
Figure 1. How to use a metered dose inhaler (MDI)
ILLUSTRATION BY JAVIER TRIGO
1: Cap should be removed and inhaler shaken to ensure consistent delivery of dose. Device should be primed if patient is using for the first time, or if not used for a while.
2: Patient should breathe out fully.
3: Patient should breathe in slowly and steadily and press down on the inhaler device.
4: On inhalation, the patient should hold their breath for a count of ten.
5: Patient should slowly breathe out, repeat dose (if applicable), and replace mouthpiece cover. Clean device if necessary after use.
Common errors in technique made by patients:
For solutions to these common errors, please see table 2.
![]()
Figure 2. How to use a metered dose inhaler (MDI) with spacer
ILLUSTRATION BY JAVIER TRIGO
1: Cap should be removed and the patient should check to see if the mouthpiece is clean. Inhaler should be shaken to ensure consistent delivery of dose. Device should be primed if patient is using for the first time, or if not used for a while.
2: The inhaler mouthpiece should be inserted into the end of the spacer device.
3: Patient should breathe in, and then breathe out fully.
4: The inhaler and spacer device should be held between the index finger and thumb. The spacer mouthpiece should be placed in the mouth, above the tongue. The patient should close their lips around the spacer device.
5: The patient should tilt their head back slightly toward the ceiling. The top of the inhaler device should be pressed to release a single dose of medicine. The patient should slowly breathe in all of the air and hold breath for ten seconds.
6: Patient should open mouth, remove spacer device and breathe out slowly. Patients could also use the tidal breathing technique, where they breathe slowly and steadily in and out four to five times.
Common errors in technique made by patients:
For solutions to these common errors, please see table 2.

Figure 3: How to use an Accuhaler
ILLUSTRATION BY JAVIER TRIGO
1: Holding the device horizontal or upright, the patient should open the inhaler by moving sliding lever in the correct direction.
2: Patient should breathe out fully but not into the Accuhaler.
3: Patient should place the inhaler device in the mouth, with the lips forming a tight seal over the mouthpiece, before breathing in quickly and deeply through the inhaler device.
4: On inhalation, the patient should hold their breath for a count of ten.
5: Patient should slowly breathe out.
6: Inhaler should be closed correctly by moving sliding lever in the correct direction. The inhaler should be cleaned as necessary.
Common errors in technique made by patients:
For solutions to these common errors, please see table 2.

Figure 4: How to use a turbohaler
SOURCE: ILLUSTRATIONS BY JAVIER TRIGO
1: The patient should unscrew the cap (turning anticlockwise) and remove. Holding the inhaler upright, the dose can be loaded by turning the coloured base to the right, as far as it will go.
2: Then twist it back to the left until it clicks. It is now loaded.
3: The patient should breathe out gently, away from the device. Holding the device without covering the air inlets, the tip of the mouthpiece should be placed between the lips and a good seal made.
4: The patient should breathe in quickly and deeply and hold their breath for 5–10 seconds. Remove the device before breathing out fully. Clean the device as necessary, replace the cap and screw it shut.
Common errors in technique made by patients:
For solutions to these common errors, please see table 2
Examples of common inhaler technique errors and recommendations for improvement are described in ‘Table 2: Common inhaler technique errors and suggested solutions’.
| Table 2: Common inhaler technique errors and suggested solutions | |
|---|---|
| Common error | Explanation and suggested solutions |
| Not shaking an aerosol inhaler device before use | Not shaking the canister properly may lead to inconsistent dosing and poorly functioning inhalers. Shake all inhalers; most dry powder inhalers (DPI) do not need shaking before use. |
| Not priming the aerosol inhaler device | Aerosol inhalers require priming (to check that the spray is functioning) before using for the first time, or if they have not been used for a while (usually five to seven days). |
| Not breathing out before inhaling | Breathing out fully (or as much as is comfortable) reduces the amount of air in the airways and increases the available space for air from the next breath. The result is a deeper than normal inhalation, maximising the opportunity to carry the drug to the site of action. |
| Incorrect positioning of inhaler device | Patients should be instructed not to hold a DPI with the mouthpiece pointing downwards during, or after loading, a dose, as the drug can escape. It should be kept horizontal or upright.
The patient should keep their chin up or head slightly tilted back when using the inhaler. It should be placed correctly in the mouth and the lips should form a tight seal over the mouthpiece. |
| Incorrect coordination of pressured metered dose inhaler (pMDI) actuation with inspiration | To deliver the medication to the lungs from a pMDI, the patient must coordinate breathing in with pressing the canister. |
| Delay in inhaling drug through a holding spacer device (a device when combined with a pMDI helps to improve aerosol delivery) | The medication stays suspended in the spacer for a short time only, so if patients fail to take each dose without delay immediately after loading the spacer, a proportion of the dose is deposited on to the inner surface of the spacer and is therefore lost. |
| Incorrect inspiratory flow rate: breathing in either too fast or too slow | The total lung deposition of an inhaled drug is strongly affected by the speed of inhalation.
|
| Not holding your breath after inhalation | The ‘breath hold’ increases lung deposition through the process of sedimentation. By keeping the air still for a few seconds, a greater number of particles will sediment on to the receptor sites because of gravity. |
| Multiple actuations without waiting in between actuations | Very rapid actuations can reduce the dose delivered per actuation. |
| Using an empty inhaler | Patients frequently fail to detect when the inhaler is empty, particularly when using reliever aerosol devices. |
| Poor maintenance of inhaler or spacer device | Spacers should be reviewed every 6–12 months to check that the structure is intact (e.g. no cracks), the outer casing is clean and the valve is functioning. |
The Pharmaceutical Journal, PJ, July 2016, Vol 297, No 7891;297(7891):DOI:10.1211/PJ.2016.20201442
Medical news and health news headlines posted throughout the day, every day.
Latest medical news and expert commentary in your specialty as well as disease information.
Medical Information and health advice you can trust
Wellness inspired. Wellness enabled.
The Pharmaceutical Journal covers analysis, features, opinion, learning and careers articles, providing insight and knowledge about drugs, pharmacy practice, medicines use and healthcare policy in the context of the pharmacy profession and pharmaceutical science.
Find information and advice on health conditions, symptoms, healthy living, medicines and how to get help (British National Health Service).
Better Information. Better Health.
Pushing the Standards of care.
No.1 Hospital in the Nation (America)
Know more. Be sure.
NORD is dedicated to supporting education, elevating care, advancing research, and driving policy for rare diseases.
Know more. Fell better.
Information on how to stay safe and healthy abroad.
Health and fitness news. Recipes, Natural Remedies
Get instant answers, find creative inspiration, and learn something new.
Into the unknown.