What is it?
Hyperkalaemia (High level of potassium in your blood) mainly due to the lack of potassium excretion from the body.
- A normal range of potassium is between 3.6 and 5.2 millimoles per liter (mmol/L) of blood.
- Degrees of hyperkalemia are generally defined as follows (however, note that not all sources agree on these levels):
-
5.5-6.0 mEq/L – Mild
-
6.1-7.0 mEq/L – Moderate
-
≥7.0 mEq/L – Severe
- The upper limit may be considerably higher in young or premature infants, as high as 6.5 mEq/L.
- A potassium level higher than 5.5 mmol/L is critically high in adults.
- Levels higher than 7 mEq/L can lead to significant blood flow changes and neurological changes, whereas levels exceeding 8.5 mEq/L can cause respiratory paralysis (breathing difficulties) or cardiac arrest and can quickly be fatal.
Diagnosis Tests
- Many patient show no symptoms and symptoms can be non specific hence testing is required whether the elevated potassium level is real or factitious.
- In a patient who does not have a predisposition to hyperkalemia, blood testing should be repeated before taking any actions to bring down the potassium level, unless changes are present on ECG. Renal function testing is important. If the patient has renal failure, the serum calcium level should be checked because hypocalcemia can exacerbate cardiac rhythm disturbances. Other tests include:
- ECG
- Urine potassium, sodium, and osmolality
- Complete blood cell count
- Metabolic profile
Measurement of the TTKG remains widely used to assess whether decreased renal excretion of potassium is contributing to hyperkalemia. Despite its initial promise, some research has called its accuracy into question. Some experts recommend that TTKG measurement be abandoned.
Depending on the clinical findings and the results of the above laboratory work, the following may be indicated:
-
Glucose level – In patients with known or suspected diabetes mellitus
-
Digoxin level – If the patient is on a digitalis medication
-
Arterial or venous blood gas – If acidosis is suspected
-
Urinalysis – If signs of renal insufficiency without an already known cause are present (to look for evidence of glomerulonephritis)
-
Serum cortisol and aldosterone levels – To check for mineralocorticoid deficiency when other causes are eliminated
-
Serum uric acid and phosphorus tests – For tumor lysis syndrome
-
Serum creatinine phosphokinase (CPK) and calcium measurements – For rhabdomyolysis
-
Urine myoglobin test – For crush injury or rhabdomyolysis; suspect if urinalysis reveals blood in the urine but no red blood cells are seen on urine microscopy
ECG
-
Vital for assessing the physiologic significance of the hyperkalemia
-
ECG findings generally correlate with the potassium level, but potentially life-threatening arrhythmias can occur without warning at almost any level of hyperkalemia
-
In patients with organic heart disease and an abnormal baseline ECG, bradycardia may be the only new ECG abnormality
-
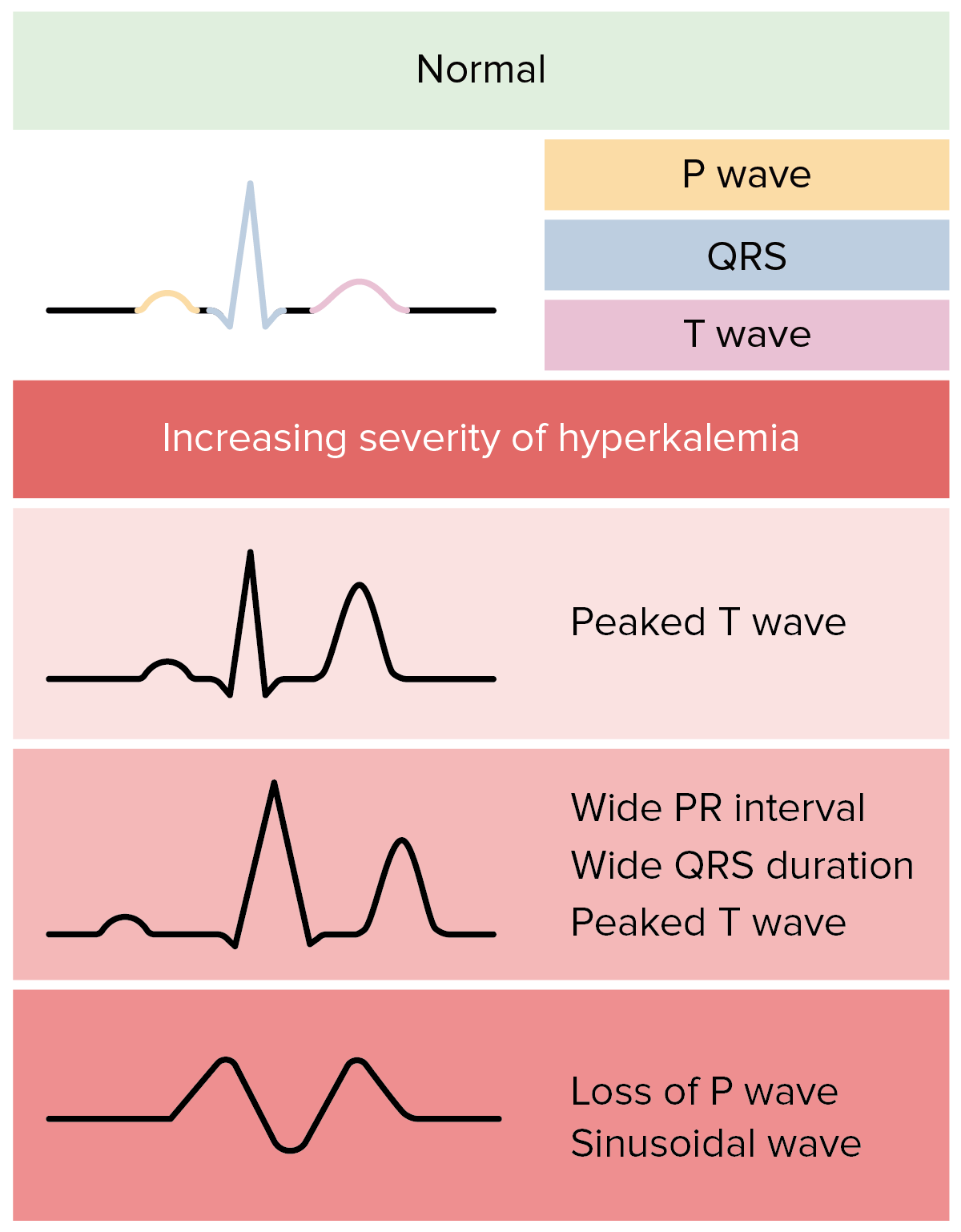
ECG changes have a sequential progression, which roughly correlate with the potassium level, but with the caveats mentioned above [2]
Early ECG changes of hyperkalaemia, typically seen at a serum potassium level of 5.5-6.5 mEq/L, include the following:
-
Tall, peaked T waves with a narrow base, best seen in precordial leads
[3]
-
Shortened QT interval
-
ST-segment depression
At a serum potassium level of 6.5-8.0 mEq/L, the ECG typically shows the following:
At a serum potassium level higher than 8.0 mEq/L, the ECG shows the following:
The progressively widened QRS eventually merges with the T wave, forming a sine wave pattern. Ventricular fibrillation or asystole follows.
Medscape
Cause
- Lack of potassium excretion from the body.
- High-potassium, low-sodium diets
- High consumption of potassium including supplements and/or medication:
- Ingestion of potassium supplements – Ingested amounts would have to be massive to be the sole cause of hyperkalemia, but even relatively small amounts can produce hyperkalemia in a patient with impaired renal excretion
- Burns and/or Injury where muscles are damaged (muscles release potassium to the blood when damaged)
- Dehydration
- High alcohol consumption
- Internal bleeding
- Absence, or very low levels, of aldosterone
- Hyporeninemic hypoaldosteronism or renal tubular disease (pseudohypoaldosteronism I or II)
- Addison’s disease
- Malignant hyperthermia
- WNK1 and WNK4 mutations
- Long term kidney disease alone generally will not cause hyperkalaemia until the eGFR is less than 20-25 mL/min.
- Kidney injury
- Kidney failure
- Type 1 diabetes
- Eating certain plants:
- Foxgloves (Digitalis purpurea and Digitalis lanata)
- Common oleander (Nerium oleander)
- Yellow oleander (Thevetia peruviana)
- Lily of the valley (Convallaria majalis)
- Squill (Urginea maritima and Urginea indica)
- Ouabain (Strophanthus gratus)
- Dogbane (Apocynum cannabinum)
- Wallflower (Cheiranthus cheiri)
Treatments
- High concentrations of potassium in IV fluid preparations (i.e. total parenteral nutrition formulas)
- Dietary salt substitutes – Several “no-salt” or “low-salt” substitutes contain about 10-12 mEq of potassium per gram of salt and can be dangerous, especially with diminished renal function
- Penicillin G potassium therapy
- PRBC transfusion (risk peaks at 2-3 weeks of cell storage)
- Cardioplegia solutions – These contain 20-30 mmol/L of potassium chloride
- Low sodium delivery to the distal tubule
Syndromes
Disorders that can cause type IV renal tubular acidosis, resulting in hyperkalemia, include the following:
Syndromes
Increased intake, this is rarely the sole cause of hyperkalaemia, because the mechanisms for renal excretion are very efficient. However, the inability to transport potassium intracellularly exacerbates hyperkalaemia in individuals who have impaired renal excretion.
Factors that can shift potassium into the extracellular space include the following:
-
-
Beta-adrenergic blockade
-
Acute tubular necrosis
-
Electrical burns
-
Thermal burns
-
Cell depolarization
-
Head trauma
Syndromes
Medication
Treatments
Vitamins, herbals and minerals
Table. Selected Factors Affecting Plasma Potassium
| Factor |
Effect on Plasma K+ |
Mechanism |
| Aldosterone |
Decrease |
Increases sodium resorption, and increases K+ excretion |
| Insulin |
Decrease |
Stimulates K+ entry into cells by increasing sodium efflux (energy-dependent process) |
| Beta-adrenergic agents |
Decrease |
Increases skeletal muscle uptake of K+ |
| Alpha-adrenergic agents |
Increase |
Impairs cellular K+ uptake |
| Acidosis (decreased pH) |
Increase |
Impairs cellular K+ uptake |
| Alkalosis (increased pH) |
Decrease |
Enhances cellular K+ uptake |
| Cell damage |
Increase |
Intracellular K+ release |
| Succinylcholine |
Increase |
Cell membrane depolarization |
- Clinical situations in which this mechanism is the major cause of hyperkalaemia include the following:
- Hyperosmolality
- Tissue breakdown (i.e. rhabdomyolysis, tumor lysis syndrome, or massive hemolysis)
- Propofol (“propofol infusion syndrome”)
- Toxins (digitalis intoxication or fluoride intoxication)
- Succinylcholine (depolarizes the cell membrane and thus permits potassium to leave the cells)
- Beta-adrenergic blockade
- Strenuous or prolonged exercise
- Malignant hyperthermia
- Hyperkalemic periodic paralysis
Medscape
Medication
- Ace inhibitors (for kidney disease and high blood pressure)
- Ace II inhibitors (for kidney disease and high blood pressure)
- The combination of spironolactone and ACE inhibitors
- Direct renin inhibitors (i.e. Aliskiren)
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Chemotherapy drugs
- Potassium-sparing diuretics, which are especially used in the treatment of cirrhosis and chronic heart failure
- Calcineurin inhibitors i.e. cyclosporine, tacrolimus)
- Antibiotics (i.e. pentamidine and trimethoprim-sulfamethoxazole)
- Epsilon-aminocaproic acid
- Oral contraceptive agents, such as drospirenone
- Pentamidine
- Trimethoprim-sulfamethoxazole
- Heparin
- Ketoconazole
- Metyrapone
Vitamins, herbals and minerals
Illicit drugs
Symptoms
- General discomfort (muscle weakness), uneasiness or ill feeling (malaise) and/or fatigue (tiredness)?
- Pain, numbness, burning and tingling (pins and needles) sensation in one’s hands and fingers (thumb and/or index finger and/or middle finger and/or ring finger and/or small finger)?
- Pain and/or numbness and/or tingling sensation in one or both legs and/or foot area?
- Sickness and nausea feeling?
- Abdominal pain and/or are constant violently vomiting or vomiting longer than than two days (one day if a child)?
- Short of breath and/or breathing difficulties?
- Chest pain and/or tight chest?
- Heart palpitations and/or irregular heartbeats?
Complications /Information to beware of/General tips:
Do not wait phone for an ambulance if one has:
Be aware of this condition if one has a:
- Slow pulse (slow heart beat -Bradycadia)
- High potassium levels
- Kidney failure
- Taking medication such as beta blockers and calcium channel blockers (verapamil and/or diazepam).
- ACE inhibitors and/or angiotensin receptor blockers (ARBs) since they may promote both renal dysfunction and hyperkalemia. Thus, the combination of an ACE inhibitor and beta blocker may set patients up for developing BRASH syndrome if they become ill for another reason (e.g., gastroenteritis).
The following foods have a high potassium level content:
- Apricots
- Avocados
- Bananas
- Bran
- Cod
- Beans and peas
- Beef
- Figs
- Kiwi
- Milk
- Nuts
- Oranges
- Potatoes
- Spinach
- Tomatoes
- Milk
- Peanut butter
Please reduce accordingly
Please talk to your healthcare professional (i.e Medical Doctor/Pharmacist) for further advice
Detailed Information
Please copy and paste any key words from the title: High Potassium levels in the following respective 'Medtick References and/or Sources' to find out more about the disease (this also may include diagnosis tests and generic medical treatments).
- Medical News Today
Medical news and health news headlines posted throughout the day, every day.
- Medscape (Professional level)
Latest medical news and expert commentary in your specialty as well as disease information.
- Healthline
Medical Information and health advice you can trust
- EveryDay Health
Wellness inspired. Wellness enabled.
- Pharmaceutical Journal (Professional level)
The Pharmaceutical Journal covers analysis, features, opinion, learning and careers articles, providing insight and knowledge about drugs, pharmacy practice, medicines use and healthcare policy in the context of the pharmacy profession and pharmaceutical science.
- NHS
Find information and advice on health conditions, symptoms, healthy living, medicines and how to get help (British National Health Service).
- WebMD
Better Information. Better Health.
- Cleveland Clinic
Pushing the Standards of care.
- Mayo Clinic
No.1 Hospital in the Nation (America)
- Drugs.com
Know more. Be sure.
- National Organisation of Rare Diseases
NORD is dedicated to supporting education, elevating care, advancing research, and driving policy for rare diseases.
- Verywell Health
Know more. Fell better.
- Fit for Travel
Information on how to stay safe and healthy abroad.
- DR Axe
Health and fitness news. Recipes, Natural Remedies
- ChatGPT (The answers here can't be verified, as it may finds answers from not the above sources)
Get instant answers, find creative inspiration, and learn something new.
- DeepSeek (The answers here can't be verified, as it may finds answers from not the above sources)
Into the unknown.